*************************************************************************************
2016/10/17 iJMAT 2015/06/27 台湾熱傷診療支援活動報告
〜 The Joint Burn Care Assistance:JMAT in Taiwan 〜
*************************************************************************************
The International Activities in Taiwan by the Joint Burn Care Assistance Team of Physicians from Japan Medical Association and Three Medical Societies
Matsuda N, Yamada S, Hinoshita T, Sasaki J, Ikeda H, Harunari N, Sakamoto T.
内容:2015年6月27日午後8時頃,台湾新北市のウォーターパーク「八仙楽園」において,カラーパウダーを使用した野外コンサートにおいて,カラーパウダーが発火し,粉塵爆発事故が発生しました。2015年6月30日において,熱傷受傷患者数は498名(最終499名),うち入院患者数は398名,うち集中治療管理患者数は277名,平均熱傷面積は44%と報告されました。私達は,日本医師会JMATとして,台湾政府からの要請に基づき,2015年7月12日(日)〜15日(水)の4日間,台湾衛生福利部(厚生労働省)および台湾医師会と連動して5つの主要施設を訪問し,熱傷診療支援を展開しました。この活動記録を,英文にまとめさせていただきました。その後,日本医師会と台湾医師会は,2015年7月30日に台北市内で「災害時の医療連携協定」を締結しました。アジアで初めての「災害医療における医療協力体制」を締結できております。
名古屋大学大学院医学系研究科 救急・集中治療医学分野 松田直之
Introduction
Cross-border medical support activities began with the Committee of Five, the predecessor of the International Committee of the Red Cross, which was established in 1863.1 In Japan, in addi- tion to the Japanese Red Cross Society, the Japan Medical Association Team (JMAT)2,3 is relied on for medical support in disaster-affected areas. JMAT was active in providing aid in the aftermath of the Great East Japan Earthquake, which struck on March 11, 2011.
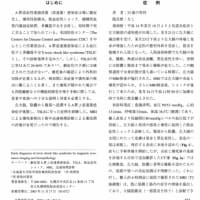
Around 8 pm on June 27, 2015, a dust explo- sion occurred at a water park called Formosa Fun Coast in New Taipei City, Taiwan, when ammable colored powder used at an event exploded. On June 30, the number of burn patients totaled 498 (ultimately there were 499 patients), of which 398 were hospitalized. Of these, 277 were intensive care patients and the average burn coverage was reported to be 44% of total body surface area.
At the request of the Taiwan Medical Asso- ciation (TMA) and the NGO Taiwan Root Medical Peace Corps (TRMPC), the Japan Medical Association (JMA) dispatched six burn experts recommended by the Japanese Society of Inten- sive Care Medicine (JSICM), the Japan Associa- tion for Acute Medicine (JAAM), and the Japanese Society for Burn Injuries (JSBI). This Joint Burn Care Assistance Team of Physicians by JMA and Three Medical Societies was in Taiwan for the four days from Sunday, July 12 to Wednesday, July 15, 2015 to collaborate with the Taiwanese government, especially Taiwan’s Min- istry of Health and Welfare, in assisting with burn treatment. This report discusses the activities of the team in Taiwan.
Preparations Leading Up to Burn Treatment Support
On June 30, JSICM began considering transport- ing burn patients by air to intensive care units in Japan. By July 7, JMA had coordinated with the TMA and Taiwan’s Ministry of Foreign Affairs, and had also brought together the JSICM, JAAM and JSBI to select six members for the team and set the procedures for sending the team. The four days from July 12 to July 15 were designated for activities, with the members serving as advisors on burn treatment but not providing direct medical treatment.
At 10:30 am on July 12, the members met at the Chubu Centrair International Airport in Nagoya, shared information on the current sta- tus of burn treatment in Taiwan, and conrmed the guidelines for their activities. On arriving at the Taiwan Taoyuan International Airport on China Airlines, representatives from Taiwan’s Ministry of Foreign Affairs and the TRMPC and reporters from many news outlets were waiting. The team then went to Taiwan’s Ministry of Health and Welfare and received information about the burn treatment following the water park accident in New Taipei City. The Ministry and the TRMPC explained the support system and schedule for the team’s stay in Taiwan (Fig. 1). The current status of the 498 burn patents (the nal count was 499) was also reviewed (Table 1).
Visits to Hospitals in Taiwan
On July 13, the team visited the Tri-Service General Hospital and the Shin Kong Wu Ho-Su Memorial Hospital, followed by the Cheng Hsin General Hospital on July 14 and the Linkuo Chang Gung Memorial Hospital and Cathay General Hospital on July 15. The team visited the ve hospitals in total that the Taiwan’s Ministry of Health and Welfare had readied for their arrival, and shared information on treatment.
Each hospital had prepared presentations on severe cases that had been difcult to manage. They shared patient information and discussed treatment and management (Fig. 2). Subsequently, the team went on hospital rounds for the burn center (Fig. 3), the critical care unit, and the hospital wards and toured the operating rooms (Fig. 4), and then thoroughly discussed the management and treatment guidelines for each patient in terms of the management of the burn wound, consciousness, breathing, circulation, infection, nutrition, regeneration and reha- bilitation. The team recognized the advanced burn treatment available at each hospital and tried to share good treatment guidelines among them. The team gave computer presentations of the burn treatment guidelines used in Japan, infection management and skin grafting with articial dermis and cultured epidermal auto- graft (CEA), and then discussed these approaches at each hospital.
All of the hospitals that the team visited were treating more burn patients than normally expected, given this emergency situation result- ing in a large number of burn patients. They all faced difculties in ensuring a sufcient number of health care providers, treatment centers for whole body management, local wound management and infection prevention.
Taiwan’s Medical Volunteer System
Regarding medical manpower, retired doctors and doctors who had started their own practices returned to the medical center as medical volun- teers to help with the treatment. In addition to these volunteers in Taiwan, if the dispatch of doctors and nurses from Japan were possible, the burden on critical care doctors could be reduced. It was determined that transporting burn patients to Japan, as considered by the JSICM, was not applicable due to the high standard of treatment in Taiwan and the strong desire and expectations of patients and their families to be treated in their own country, as well as the risks associated with wide-area transport.
Bedside Discussions on Whole-body Management
All of the ve hospitals used the same approach to whole-body management as Japan uses in its burn treatment. However, not all of the doctors treating patients with multiple burns were expe- rienced in burn treatment. The team was thus able to serve as intermediaries between doctors specializing in burn treatment and doctors with other specialties.
First, the team gave a presentation on the effective use of dexmedetomidine (DEX) for pain relief and mitigation, and shared informa- tion on the relationship between pain manage- ment and maintaining immunity. DEX4,5 is an α2 adrenoreceptor agonist widely used in Japan during the intensive care phase. In addition to a sedative effect via the locus ceruleus, DEX is effective in easing pain in the trunk of the body. The team discussed the effect DEX could have in easing sympathicotonia, as well as stabilizing circulation.
As regards respiratory care, the dust explo- sion caused by the corn starch used in the col- ored powder resulted directly in airway burns, lung injuries and accompanying respiratory infections in some patients. The inhalation burn injury6 caused by the dust explosion required attention and careful follow-up. As a result of the respiratory tract injuries caused by burning corn starch adhering to the trachea, extracorpo- real membrane oxygenation (ECMO) was intro- duced. There have been cases in which patients could be removed from ECMO. There were over 20 cases in each hospital of patients requiring articial respirators for pulmonary edema as a result of this kind of airway burn and mass trans- fusions required to manage extensive burns.
In cardiovascular management, there was a general understanding about the difculty of managing the initial transfusions in the many symptoms present when burns cover more than 40% of the body. The team discussed manage- ment guidelines for uid therapy in the case of severe inammation, as seen with sepsis and burns, including an approach to restoring uid balance using pulse pressure variation (PPV) and stroke volume variation (SVV) for wave- form analysis of pulse waves,7-9 and circulation management through ultrasound scans. In addi- tion, we discussed treatment guidelines for cases in which cardiac tamponade and large-volume pleural effusion, which can occur with transfu- sions in extensive burns, function as restrictive factors for the heart and thus impede circulation. In conrming these individual cases, treatment guidelines were discussed at the bedside and treatment guidelines were shared.
Management of Burn Wounds
Even 16 days after patients had rst received the burns, there were several cases in which debride- ment of the burn wounds was not yet complete. Since the objective was to save the lives of the many patients with extensive burns, an approach was used in which debridement in a small area was carried out over several days and repeated while the patient was under general anesthesia. There were several severe cases, which were required escharotomies due to circumferential deep burns.
At each hospital, the team explained the gen- eral process for burn treatment, the target time for completion of debridement, wound treat- ment, methods for cleaning wounds, and the use of topical agents, and shared information on treatment management. The team also gave pre- sentations using computers on the use of cul- tured epidermal autograft (CEA) combined with auto 6 to 1 meshed split thickness skin graft called hybrid method in Japan. In these presen- tations, the method using CEA, which is not yet approved in Taiwan, the “sandwich” method in which articial dermis and autologous skin are combined, negative pressure wound therapy, and a method using silver sulfadiazine were dis- cussed, and treatment guidelines were shared.
Management of Infection and Sepsis
There were cases in which local infection and respiratory tract infections resulted in sepsis. In addition to enteric bacteria, pathogenic bacteria such as Acinetobacter baumannii, Methicillin- resistant Staphylococcus aureus, Pseudomonas aeruginosa and Candida spp. were causing prob- lems, and multi-drug-resistant Acineobacter infections were conrmed in particularly high numbers. The team shared information about the status of the management of multi-drug-resistant bacteria in Japan and effective monitoring of bactericide blood concentration levels, as well as the effectiveness of measuring plasma (1→3)-β-D-glucan10 in managing fungi and the appropriate use of antifungal agents.
Coordination with Taiwan’s Ministry of Health and Welfare
After visiting the hospitals, the team stopped by the Ministry of Health and Welfare every day to report on the status of burn management at the hospitals and share information on its activities. The Ministry considered the use of CEA, which was approved for manufacture by Japan’s Ministry of Health, Labour and Welfare as Japan’s rst human cell/tissue-engineered medical device (product name: JACE®, Japan Tissue Engineering Co., Ltd., Japan)11 on October 29, 2007. In addi- tion to describing the characteristics of CEA and the pros and cons of its use, the team provided specic information on whole-body management, such as the exact skin grafting methods for burns (burn management using articial dermis and CEA that has been preserved), optimizing debridement, wound management using negative pressure wound therapy, methods for clean- ing wounds, infection and sepsis management, and pain management and mitigation. Files of the presentations given by the team were pro- vided to the Ministry of Health and Welfare and the respective hospitals via the TRMPC.
In Closing
The Joint Burn Care Assistance Team’s work in Taiwan conrmed the need for medical collabo- ration between Taiwan and Japan in accidents resulting in multiple casualties. The visits to the ve representative hospitals—the Tri-Service General Hospital, the Shin Kong Wu Ho-Su Memorial Hospital, the Cheng Hsin General Hospital, the Linkuo Chang Gung Memorial Hospital and Cathay General Hospital—afrmed the effectiveness of treatment collaborations in emergency situations. The team informed the JMA and Taiwan’s Ministry of Health and Welfare of the need to establish a mutual sup- port system in both countries to respond to multi-casualty events in Taiwan and Japan. Discussions with medical professionals from Taiwan’s Ministry of Foreign Affairs, Ministry of Health and Welfare, the TMA, the TRMPC and others (Fig. 1) demonstrated the importance of medical interaction between the two countries.
Acknowledgments
We would like to express our deep gratitude to Yoshitake Yokokura (JMA), Masami ISHII (JMA), Tetsuo Yukioka (JAAM), Yoshihito Ujike (JSICM), Hiroaki Nakazawa and Hajime Matsumura (JSBI), the JMA, JSICM, JAAM, JSBI, TMA, the Taiwanese government, especially the Ministry of Health and Welfare, and TRMPC for the support given during our stay in Taiwan. We are grateful for the opportunities to exchange views with representatives from the TMA and Taiwanese government and the chance to give an optimistic report on the direction of joint medical support. Moreover, we are sincerely grateful to everyone at the Tri-Service General Hospital, the Shin Kong Wu Ho-Su Memorial Hospital, the Cheng Hsin General Hospital, the Linkuo Chang Gung Memorial Hospital and Cathay General Hospital, and Yen Ta Huang (Tzu Chi University), who took time from their busy schedules to have such fruitful discussions with us. We are praying for the recovery of ev- eryone hurt in this incident.
References
1. International Committee of the Red Cross. https://www.icrc.org/ eng/who-we-are/history/overview-section-history-icrc.htm.
2. Ishii M. Activities of the Japan Medical Association Team in response to the Great East Japan Earthquake. JMAJ. 2012; 55(5):362-367.
3. Ishii M, Nagata T. The Japan Medical Association’s disaster pre- paredness: lessons from the Great East Japan Earthquake and Tsunami. Disaster Med Public Health Prep. 2013;7:507-512.
4. Hoy SM, Keating GM. Dexmedetomidine: a review of its use for sedation in mechanically ventilated patients in an intensive care setting and for procedural sedation. Drugs. 2011:30;71:1481- 1501.
5. NelsonS,MuzykAJ,BucklinMH,BrudneyS,GagliardiJP.Den- ing the role of dexmedetomidine in the prevention of delirium in the intensive care unit. Biomed Res Int. 2015;2015:635737.
6. Beausang E, Herbert K. Burns from a dust explosion. Burns. 1994;20:551-552.
7. Pinsky MR. Functional haemodynamic monitoring. Curr Opin Crit Care. 2014;20:288-293.
8. Hofer CK, Cannesson M. Monitoring uid responsiveness. Acta Anaesthesiol Taiwan. 2011;49:59-65.
9. Matsuda N. Treatment strategy for sepsis and septic shock. The Journal of the Japan Medical Association. 2016;144:2031-2035. (in Japanese)
10. Weiss E, Timsit JF. Management of invasive candidiasis in non- neutropenic ICU patients. Ther Adv Infect Dis. 2014;2:105-115.
11. Japan Tissue Engineering Co., Ltd. http://www.jpte.co.jp/english/.
Figures & Table

The Joint Burn Care Assistance Team’s visit to Taiwan was carried out in collaboration with the Taiwan Medical Association (TMA) and Taiwan’s Ministry of Foreign Affairs. The need to set up a medical system for emergencies, such as wide-area disasters was discussed. In addition, it was confirmed that there is the need to establish legislation through collaboration between the TMA and JMA for emergency medical support systems.

Figure 2. Presentations and discussions on severe symptoms
This is an image of discussions of cases at the Shin Kong Wu Ho-Su Memorial Hospital on July 13, 2015. The situation was tense as the patient’s symptoms were extremely severe. In addition to presentations on cases of severe burns using computer projections and discussions of treatment guidelines, the team visited the rooms of patients with severe injuries and reviewed treatment guidelines on an individual basis in conjunction with the symptoms in each case.

Figure 3. Making the rounds of the burn management unit
This is a picture of the team making the rounds of the burn center and the beds in the intensive care unit at the Tri-Service General Hospital on July 13, 2015. The treatment guidelines for individuals were discussed in conjunction with their symptoms, and treatment information was shared.

Figure 4. Tour of operating room and specific advice on operations
At the Cheng Hsin General Hospital on July 14, 2015, the team discussed surgical guidelines in the operating room. Debridement of burn wounds, cleaning of wounds and infection management were discussed in full to arrive at management guidelines.
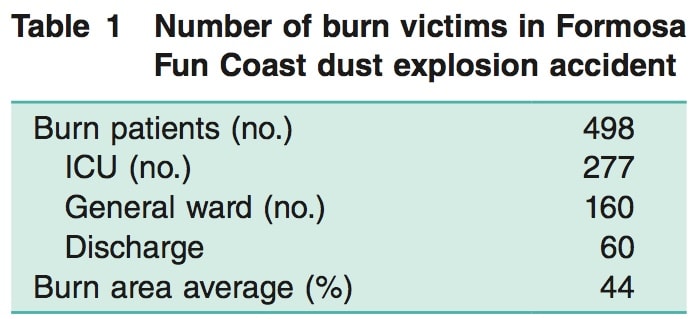
Table 1. Number of burn victims in Formosa Fun Coast dust explosion accident
This is the breakdown of the injured as announced by Taiwan’s Ministry of Health and Welfare on June 30, 2015. Initially, 277 patients were in intensive care units. Subsequently, one more person was added and the number of injured was revised to 499. The average burn coverage was about 44%. Of these, 11 people (2.2%) had died as of August 13, 2015, which is an extremely high rescue rate.
JMAT Agreement 日本医師会による日台医療連携締結 2015/07/30