講座 急性肝不全の管理 2016
名古屋大学大学院医学系研究科
救急・集中治療医学分野
松田直之
はじめに
肝不全は,広範な肝細胞死から肝臓における蛋白合成や解毒能が低下し,生命維持に障害をきたす病態です。消化管から門脈を介しての肝血流の流入が減じ,それらの肝臓以外への静脈系短絡により,門脈圧は正常な5-10 mmHgから上昇し,門脈圧亢進症が生じ,食道静脈瘤,直腸静脈瘤やメズサの頭(腹壁静脈瘤)のように,消化管出血や静脈瘤破裂に注意が必要となります。消化管からの吸収された分子が門脈を通して肝臓に移行しなくなるため,肝臓の1st pass effectが低下し,肝解毒能などの低下などにより,意識障害として肝性脳症が生じることにも注意します。
この肝不全は,急性型である急性肝不全と,慢性型である肝硬変に大別されます。欧米における急性肝不全(acute liver failure:ALF)は,従来の日本における肝炎ウイルスによって病理学的に肝炎像が進行する劇症肝炎(fulminant hepatitis:FH)に限らず,肝炎像を伴わない肝不全として例えば,急性循環不全,急性薬物中毒,妊娠,Reye症候群などを含むものとして定義されています。これに照らして,本邦においても急性肝不全の診断基準が2011年に厚生労働省「難治性の肝・胆道系疾患に関する研究班」より公表され,2015年に改定されています1,2)。右心不全やショックの遷延によっても,また,薬物中毒や熱中症においても,肝不全は生じます。
このような急性肝不全においては,ウイルス性肝炎や右心不全などの要因を明確として,早急に治療指針を立てる必要があります。急性期には,集中治療管理や全身管理が必要となる場合がありますが,その見極めとなる内容を整理できると良いです。本稿では,急性肝不全の診断と治療,そしてショック肝の管理についてまとめます。そして,時期を見て,時折,追記とさせていただきます。
急性肝不全の本邦における定義
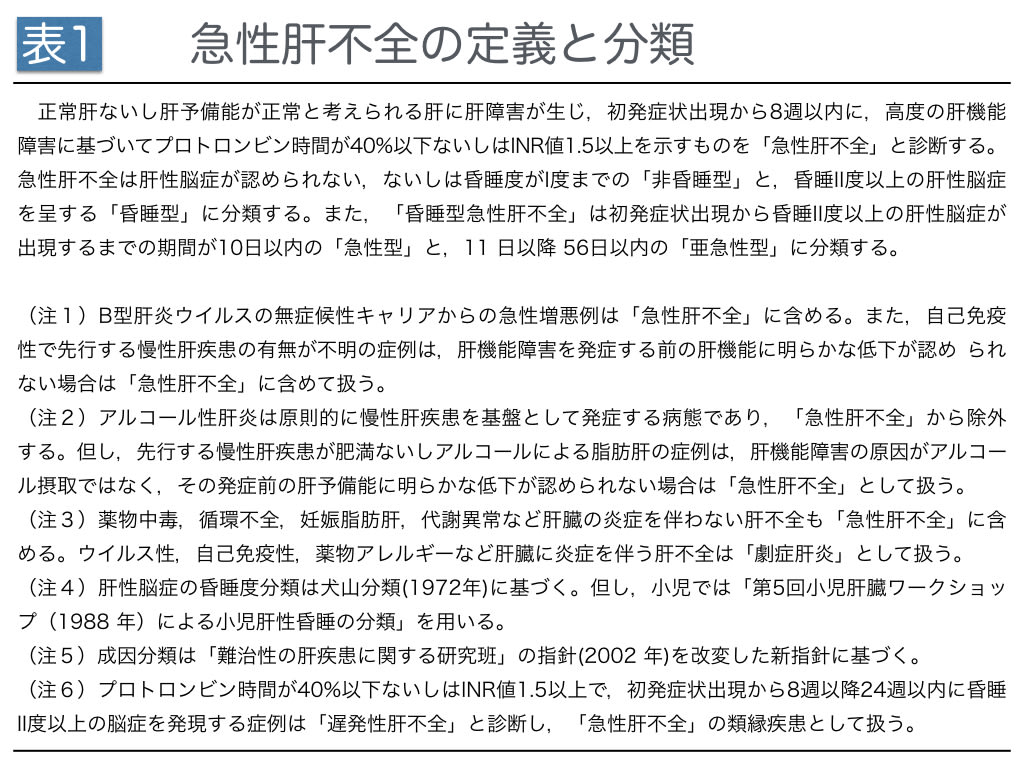
急性肝不全の定義と診断基準は,2011年に拡大されており,本邦では「難治性の肝・胆道疾患に関する調査研究」班の研究報告1,2)が知られています。2016年の段階で,急性肝不全の定義は,「正常肝ないし肝予備能が正常と考えられる肝に肝障害が生じ,初発症状出現から8週間以内に高度の肝機能障害に進行し,プロトロンビン時間(prothrombin time:PT)が40%以下あるいはPT-INR値1.5以上を示すものとされています(表1)。
肝臓の機能というと,GOTとGPTが上昇する病態と答える学生さんがいますが,肝臓の機能として大切なことは,①蛋白合成,②凝固因子産生,③コレステロール合成,④解毒能です。血清蛋白のうち最も多いアルブミン,抗凝固に関与するアンチトロンビンⅢ,副交感神経や神経筋接合部の活性分子アセチルコリンの分解するコリンエステラーゼなど多くの蛋白を産生しています。
急性肝不全における意識障害は,肝性脳症が昏睡度としてI度までの「非昏睡型」と,昏睡II度以上の肝性脳症を呈する「昏睡型」に分類されています。また,昏睡型急性肝不全は,初発症状出現から昏睡II度以上の肝性脳症が出現するまでの期間が10日以内であれば「急性型」,11 日以上 56日以内までとして「いいゴロ」が見つかりませんが「亜急性型」に分類しています。
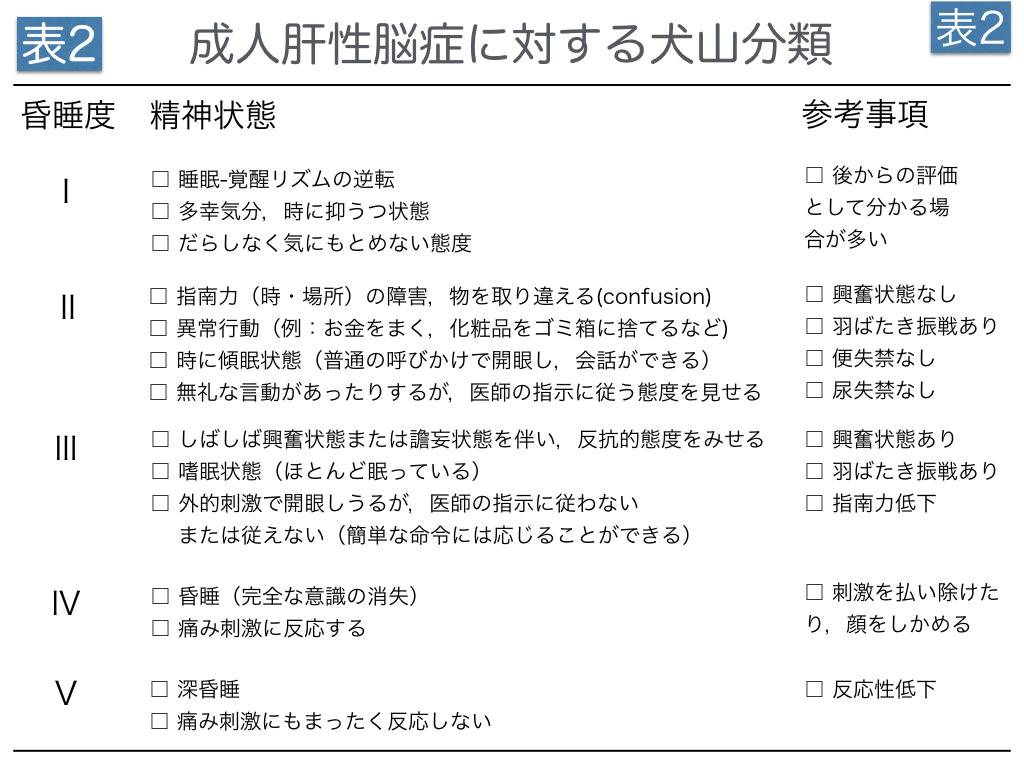
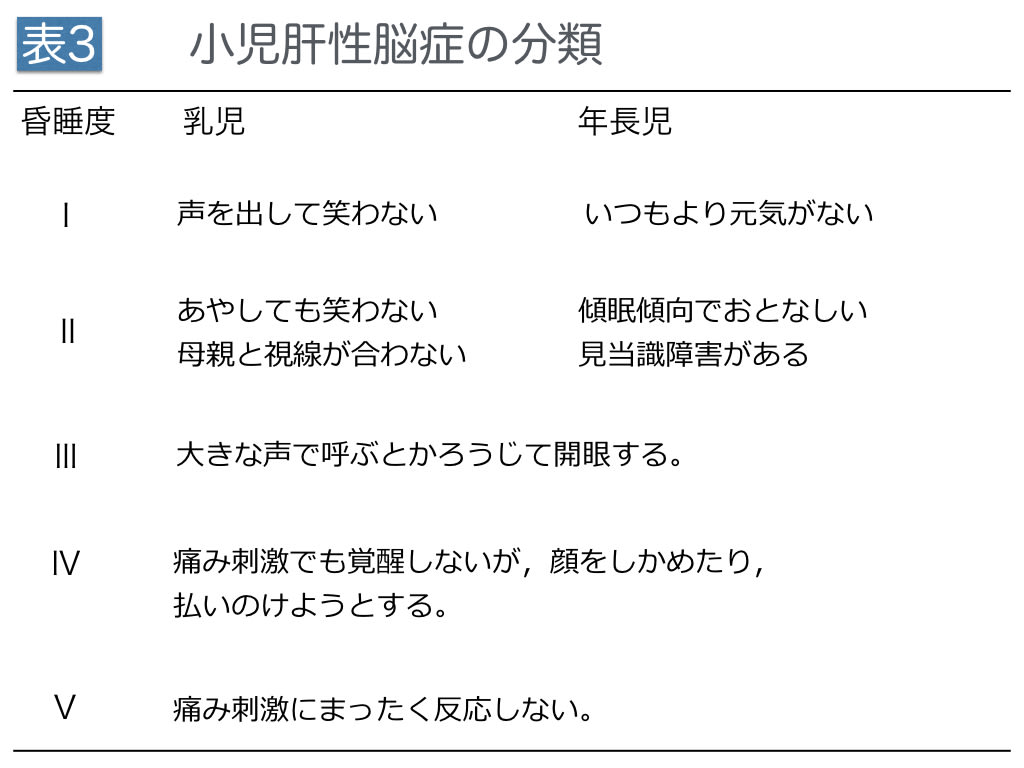
一方,肝性脳症における昏睡度の判定には,成人では犬山分類(表2)3)が現在も用いられています。劇症肝炎は,例えば,肝性脳症Ⅱ度以上,初発症状の出現から10日以内の昏睡の発症として,急性昏睡型肝不全に分類できます。また,小児では「第5回小児肝臓ワークショップによる小児肝性脳症の分類」(表3)が用いられています。日本における小児劇症肝不全の発生数は,2016年までの段階で年間約10〜20例であり,成人劇症肝炎の年間約1,000例と比べると非常に少ないという特徴があります。
急性肝不全の発症原因の評価
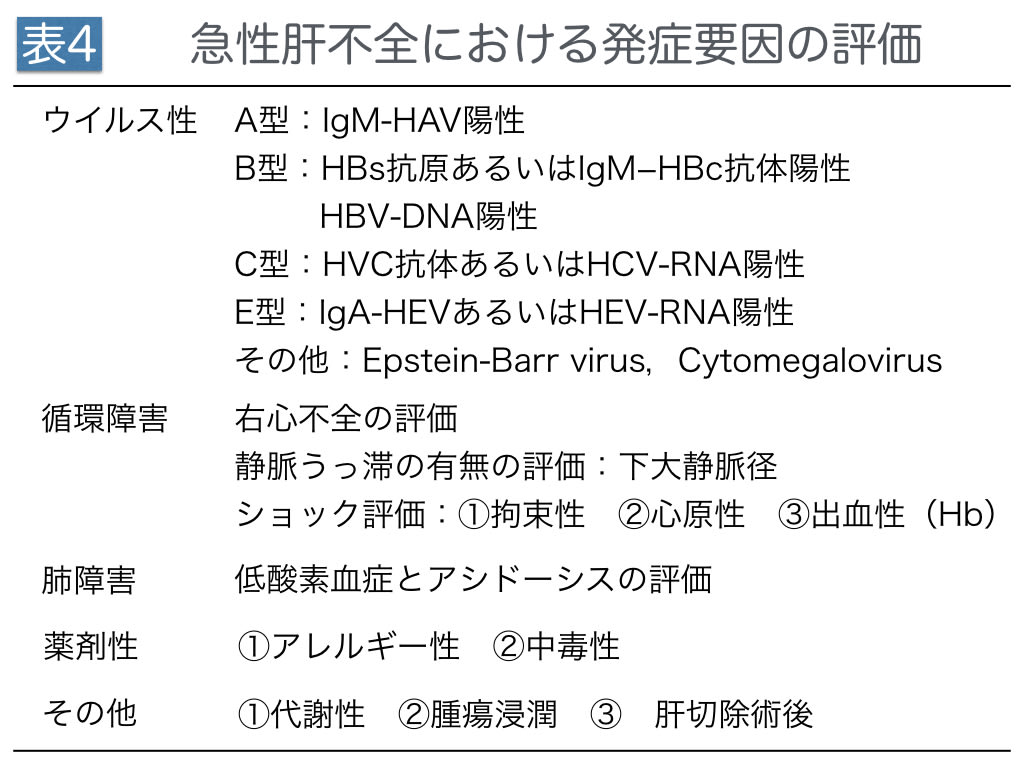
急性肝不全においては,発症に関与する要因の評価が必要です(表4)。要因,この原因についての治療は炎症の進行を抑制するために不可欠となります。急性肝不全の治療では,2次的な増悪を抑制するために「呼吸と循環の安定化」に注意しますが,付け加えてウイルス性要因と薬剤性要因の評価を行ないます。ウイルス性要因については,IgM-HAV,HBs抗原,IgM−HBc抗体,HBV-DNA,HVC抗体,HCV-RNA,IgA-HEV,HEV-RNA,およびEpstein-Barr virus(EBV),サイトメガロウイルス(Cytomegalovirus:CMV)の評価を行っています。
EBVに対する抗体は,外殻抗原(viral capsid antigen:VCA),核内抗原(EBV- associated nuclear antigen:EBNA),早期抗原(Early Antigen:EA-DR)の3種の抗原をターゲットとする抗体を評価します。早期抗原EAには,アルコール非感受性のEA-Dとアルコール感受性EA-Rがあり,合わせてEA-DRと呼ばれています。EBVウイルスが溶解感染を起こした時にVCAとEA-DRが発現することが知られており,一方,EBNAは潜伏感染において発現するようです。EBVは伝染性単核症の原因ウイルスとして特に有名ですが,この急性期などのように,IgM-VCA抗体が出現する場合,EBV感染の確定診断となります。また,IgG-VCA抗体はEBVの既感染状態で陽性となりますが,感染増悪,すなわち再活性化により異常高値となりますので,IgG-VCA抗体の異常高値においてはEBV感染の増悪を疑います。その上で,EBNA抗体は初感染の回復期から陽性になり,持続的に検出される傾向があることに注意します。以上より,急性肝不全におけるEBVの評価4)としては,IgM-VCA抗体とEBNA抗体または,IgG-VCA抗体のペア血清とEBNA抗体を検査します。再活性化したEBVに対してはIgG-VCA抗体や IgG-EADR抗体を評価します。保険未収載ですが,血液中のEBV量を定量できます。
そして,CMVが肝炎を誘導することも知られています5, 6)。CMVにおいては,IgG-CMV抗体は既感染,IgM-CMVは新規感染として評価する。ウイルス迅速同定にはシェルバイアル法,CMV抗原血症検査としてCMVアンチゲネミア法,さらに尿,血液,唾液,骨髄液,BAL液など各種検体からCMVのDNA定量を行います。
呼吸および循環が肝不全に与える影響については,肝臓や全身の虚血の評価が重要です。全身や肝臓の低酸素を導く要因は,①低酸素血症,②貧血(Hb<7 g/dLに注意),③静脈うっ血(拘束性ショック,右心不全),④低心拍出量・低血圧であり,適時,代謝性アシドーシスの進行(base excess)と血清乳酸値推移を動脈血ガス分析で評価し,時系列での虚血評価の中で肝不全の治療を展開します。その上で,薬剤性要因などにおいては,その早急な代謝を考慮することが必要です。また,自己免疫に関する評価も必要となります。
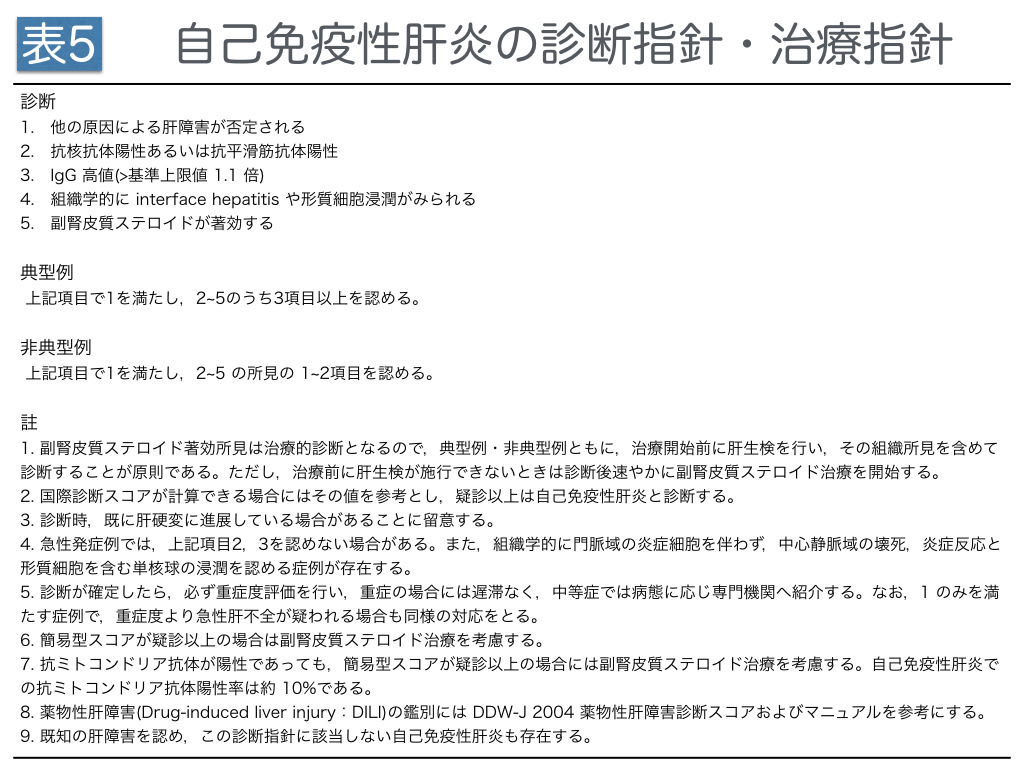
自己免疫性肝炎は,自己抗体の検出パターンで 1型と2 型に分類されています。本邦では1 型が多く,抗核抗体または抗平滑筋抗体が陽性となる特徴があります。2 型は抗 LKM-1 抗体が陽性となる特徴があり,欧米の若年層に多く,本邦では少ないとされています。 自己免疫性肝炎については,1型における抗核抗体や抗平滑筋抗体,2型におけるLKM-1やPD-1などの自己抗体の陽性,血清IgGの高値を確認します。日本人では約60%の症例でHLA(human leukocyte antigen)-DR4陽性,欧米ではHLA-DR3とHLA-DR4 の陽性例が多いことから,これらの自己抗体の発現には遺伝的素因が関与していると考えられています。本邦における「難治性の肝・胆道疾患調査研究班」による全国集計では約1,000名が自己免疫性肝炎として登録されており,約10,000名の自己免疫性肝炎が本邦に存在すると推定されています。本邦の自己免疫性肝炎は,50〜60歳代の女性に発症し,慢性肝炎となりやすいことも知られています7, 8)。自己抗体に対しては,ステロイドで効果的に抑制できる可能性があります(表5)。
一方,小児肝不全の発症要因としては,先天性心疾患などによる心不全要因に加えて,B 型肝炎や単純ヘルペスの母児感染例における抗ウイルス薬投与,自己免疫性肝炎,血球貪食症候群などが知られています9)。幼少時期には,感染症として単純ヘルペスウイルス,アデノウイルス,エコーウイルス,コクサッキーウイルスなどのウイルス感染症,先天代謝異常として,新生児ヘモクロマトーシス,ミトコンドリア脳筋症,果糖不耐症,α1アンチトリプシン欠損症,ガラクトース血症,チロジン血症,Zellweger症候群(ペルオキシソーム形成異常)などに注意が必要となります。学童期以降は,熱中症,バルプロ酸,アセトアミノフェン,サリチル酸などの薬剤性肝障害,自己免疫性肝障害,Wilson病などによる肝不全に注意します。
急性肝不全の管理
急性肝不全では,肝細胞死に伴う肝細胞やミトコンドリアから放出される細胞壊死分子が全身性炎症を導きます10-12)。これらは,近年はdamage-associated molecular patterns(DAMPs)12)として概念が整理されてきていますが,全身性炎症として急性肺傷害,ショック,急性腎傷害,播種性血管内凝固(disseminated intravascular coagulation:DIC)を誘導します。急性肝不全では,このような肝細胞死に伴う2次性に多臓器不全の誘導が起こりますし,直接に肝性脳症による意識障害,門脈圧亢進に伴う心前負荷上昇,消化管浮腫とbacterial translocation,胸水および腹水などの3edスペース形成,脾機能亢進に伴う血小板減少症なども導かれ,このような「肝臓の急性虚血」の表現型として「ショック肝」という呼称が用いられます。
1. 感染防制御の多職種間における徹底
急性肝不全の管理においても,他の急性期病態と同様に,接触感染予防策の徹底が必要です。血液浄化法に用いる挿入したカテーテルや中心静脈路に対する接触感染は,特に予防に注意すべきです。急性肝不全における予防的抗菌薬については,現在までに推奨するエビデンスはありませんので,予防的抗菌薬の投与を推奨していません。急性肝不全では,呼吸数が速く交感神経緊張のあるときなどは特に,好中球やリンパ球の機能が低下します。易感染状態にあることに注意し,感染兆候の出現した際には,血液培養検体を直ちに2セット以上提出し,グラム陽性菌およびグラム陰性菌を念頭においた広域抗菌薬を治療的抗菌薬として投与するようにします。
2.意識・呼吸・循環の安定化
意識・呼吸・循環の安定化は,併行して三位一体として対応します。急性肝不全では,まず肝性脳症の昏睡度(表2)を評価し,頭蓋内圧(intracranial pressure:ICP)の上昇に注意した管理とします。特に肝性脳症Ⅲ度以上では脳還流圧(>60 mmHg;70 mmHgを推奨)を維持することが大切です。平均血圧80 mmHgで管理していれば,ICP 20 cmHgの時に脳還流圧はギリギリ60 mmHgとなります。脳浮腫状態としてICPが上昇している状態では,原因となる昏睡惹起分子を血液濾過(hemofiltration:HF)で補助的に除去することを検討する一方で,適切に鎮静し,グリセオール(200 mL, 1日3回投与)などでICPを低下させるようにします。
ICPモニタリングを安全に施行できると良いですが,血小板数や凝固因子産生の低下のための出血合併症として安全管理面での賛否両論があり,頭部CT像や瞳孔径で代用することが多いのが実状となっています。成人における急性肝不全の鎮静については私は,呼吸数20回/分以下を目標としたフェンタニール持続投与による交感神経緊張の緩和,デクスメデトミジン持続投与(0.2-0.7μg/kg/時)によるせん妄と不穏の抑制,昼夜の覚醒リズム作成としてラメルテオン内服(8 mg PM8:00),プロポフォール持続投与の併用(30-100 mg/時:夜間PM10:00-朝方AM6:00)をお勧めしています。交感神経緊張の変動は,①呼吸数変動,②心拍数変動,③リンパ球数変動などで日々のモニタリングとしています。その上で,鎮痛と鎮静については,日本集中治療医学会などの鎮痛・鎮静ガイドラインなどを参考とし,Richmond Agitation-Sedation scale(RASS)などの鎮痛鎮静スケールを用いた適正管理とし,人工呼吸管理中はspontaneous breathing trial(SBT)を必須とし,日内変動として昼夜の生体リズムを持たせることを重視するように指導しています。
以上において,適切な交感神経緊張抑制に対する呼吸補助策として,まずhigh flow nasal cannula(HFNC)(流量45 L/分)を併用し,無気肺の軽減,吸入期酸素濃度の低下に役立てるとよいでしょう。また,マスクによる用手的換気補助や気管挿管においては,ICP上昇に対すて,十分に注意してください。30 cmH2Oを超える気道内圧により,脳浮腫を助長してしまう可能性があります。吸痰時などのために,ジャクソンリース回路での加圧,吸痰時のファイティング,気管支鏡による吸痰での咳反射,高いpositive end-expiratory pressure(PEEP),硬便の排便などに注意が必要な状態です。
循環管理については,低蛋白血症や血管透過性亢進により,血管内ボリュームが維持しにくい一方で,上大静脈領域と下大静脈領域での血流分布に異常が生じてくる場合もあります。このような循環管理において大切なことは,パルスオキシメータや観血的動脈圧におけるパルス波の観察とエコーによる適時評価です(2008年1月3日:救急一直線:講義 パルスオキシメータおよびA-lineの圧波形の読み方)。胸水,心嚢液などは,拘束性要因として,急性肝不全をショック肝に移行させやすい因子ですし,無気肺を進行させる可能性がありますので,十分に注意することが必要です。
3.ショック肝の阻止
心臓の肝臓に与える因子として,心拡張能に十分な注意が必要である。集中治療管理では,適時,心エコーを行い,心嚢液,心前負荷,心機能を評価します。心拡張能を傷害させる因子として注意が必要なものは,①拘束性要因(大量胸水,気胸,心嚢液),②心筋細胞の細胞内カルシウム過負荷(pH低下,低体温,アドレナリン作動性β受容体刺激,慢性心不全,交感神経緊張),③肺高血圧(肺血栓塞栓症,肺動脈内皮細胞傷害を含む)です。血圧低下を来し,虚血としてショックが遷延した際にも,急性肝不全が進行し,ショック肝となります。このため,ショックに関しては1時間を目安としてできる限り速やかにショックを離脱することが必要です。また,pH低下におけるドブタミンなどのβ受容体刺激薬の使用は,心拡張不全を誘発する可能性があり,注意が必要です。一方,ショック肝として,肝逸脱酵素の3桁以上への急上昇を認めた際には,肝臓のミトコンドリア等のDAMPsの希釈と排泄として,適切な輸液とし,利尿を「原尿」として維持することが必要です。このような状態では多くの炎症性リガンドが血中および組織内で濃度を高めており,炎症性多臓器不全の併発を緩和させる工夫が必要です。カテコラミンとして併用するのは,体血管抵抗を調節する目的としてのノルエピネフリン(0.05〜0.2μg/kg/分)であり,極めて心機能が低下している場合にのみアドレナリン(0.07~0.2μg/kg/分)を考慮します。これらは,少量から緩徐に増量して用いることを原則とし,絶えず減量するように試みることが大切です。
4.腎管理と血液浄化法
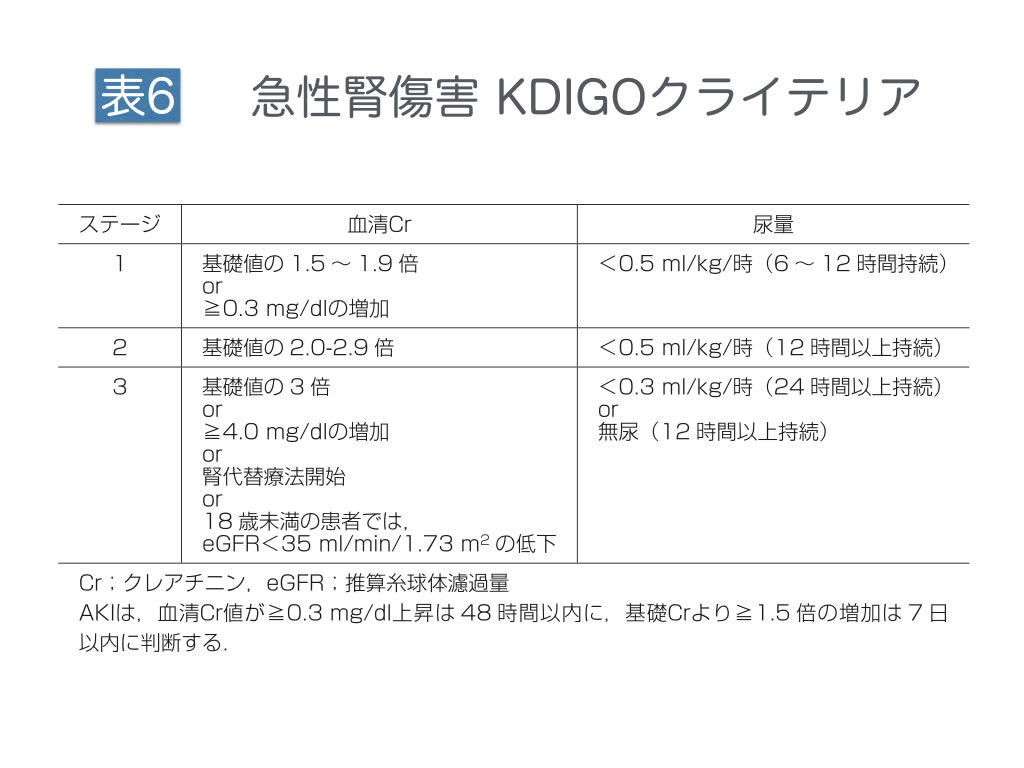
急性肝不全は,炎症性リガンド,DAMPs反応,腎静脈うっ滞(腎後負荷増大),心拡張不全などの要因により,急性腎傷害(acute kidney injury:AKI)を合併しやすい病態です。上述の方法で,意識・呼吸・循環を安定させる過程で,尿量0.5/kg/分を維持できるように管理します。
AKIの進行は,Improving Global Outcomes(KDIGO)分類13, 14)などに準じて,尿量0.5/kg/時に維持を目標とし,クレアチニンの変動として評価します。この際に,フロセミドは,ループ利尿薬として尿細管再吸収を抑制するものであり,心前負荷や肝腎後負荷を軽減する上では有効ですが,炎症や増殖性病態の管理には不適切であることに注意します。急性肝不全の急性期においても,適切な心前負荷のない状態でのフロセミドは,インターロイキン-6などの炎症性分子やTGF−βなどの線維芽細胞増殖作用分子を蓄積させる可能性があり,注意が必要です。また,炎症期や増殖期のうっ血に対しては,ヒト心房性ナトリウム利尿ペプチド(hANP:0.02μg/kg/分レベル)を併用することをお勧めしています。
利尿については,尿浸透圧と尿中クレアチニン排泄を評価する過程で,有効な濾過を維持することが大切です。このような原尿維持ができていない場合は,持続濾過(continuous hemofiltration:CHF)とし,20 mL/分あるいは30 mL/分の濾過として,腎臓の濾過機能を補助するようにします。意識障害が著明なときには,high volume CHFとして,約8時間で40Lの濾過を計画します。私は,膜面積2.1 m2,血流速度 500 mL/分,100 mL/分の濾過により,50kDa以下の中分子と小分子を通常の腎機能レベルに除去する方法を用いています。このろ液量に対する補液として,血漿交換のように新鮮凍結血症(fresh frozen plasma:FFP)を用いる場合もあります。また,アンモニアなどの小分子の除去を中心とする場合は,high flow hemodialysis(HD)を併設し,high volume high flow HDFとする場合もあります。しかし,このような意識改善のためのhigh volume high flow HDFは,肝細胞崩壊やアンモニアの再分布の時系列に影響を受けるため,意識改善までに少なくとも3日以上の施行を必要します。
一方,長期管理として慢性腎不全に移行した場合に,腎性貧血としてエポジン®(エリスロポイエチンβ)などのエリスロポイエチン製剤を併用する場合があります。エリスロポイエチンは分子量約30kDaの糖蛋白です。PMMA膜やPMX-DHPなどの一部の血液浄化膜に吸着されること15)に注意が必要です。慢性透析患者さんに対して,エポジン®であれば通常は6,000国際単位を1週間毎に使用しますが,これは間欠的HDにおける一つの指標です。持続濾過CHFの場合には,濾過流量が20 mL/分であれば,通常量のエポジンは約5日で濾過されますし,使用している膜がPMMA膜であれば約2~3日で血中より消去される可能性があります。
5.凝固・線溶系の管理
急性肝不全においては肝臓での凝固因子産生が低下するために,出血合併症に注意し,フィブリノゲン,PT-INRおよびAPTT比を1.5以下の管理としてFFP)を補充します。一方,炎症により線溶系は抑制されるため,フィブリン分解産物(FDP)やD−ダイマーは,炎症の急性期では一般に異常高値とはなりません。一方,腹水や胸水がある場合には,フィブリノゲンが腹水中や胸水中に漏出するため,血中にFDPとして再分布し,FDPが高値となります。このように,FDPはフィブリノゲン分解産物(1次線溶)とフィブリン分解産物(2次線溶)の両者を反映しますが,D-ダイマーはフィブリン分解産物(2次線溶)の最小単位ですので,血性でない限りは腹水や胸水に影響されにくい特徴があります。FDPがD-ダイマーに比べて有意に高値である場合には腹水量や胸水量をエコーなどで評価することでアセスメントとします。
FFPの補充については,循環血液量と循環血漿量を考えます。循環血液量を,エコーで推定することもお勧めします。循環血漿量は,循環血液量としての約70 mL/kgに(1−ヘマトクリット値/100)をかけたものですので,一般には約40 mL/kgレベルです。このため,凝固因子の血中濃度を約20~30%上昇させるのに必要な新鮮凍結血漿(FFP)は,理論的には8~12 mL/kg(40 mL/kgの20~30%)です。60 kgレベルであれば4単位(800 mL血液分)レベルとなると思います。以上を含めて,急性期には出血合併症を生じないレベルのフィブリノゲン,PT-INRおよびAPTT比を凝固検査として提出し,FFPの1日使用量を時系列で評価していきます。
また,全身性炎症に伴い,肝臓,脾臓,肺を含めて全身性に血管内皮に血小板が沈着し,急激な血小板減少が生じます。このような凝固亢進期では,トロンビン活性が高まることで,アンチトロンビン(AT)活性が低下しやすい状態となります。急性肝不全に伴う肝臓でのAT産生低下に加えて,炎症性にAT消費が進むため,肝内凝固や脾内凝固,さらには様々な血管内皮細胞傷害の抑制のためにATやリコンビナントトロンボモジュリンを補充する場合があります。AT補充については,全身性血小板沈着を抑制することを目標とした播種性血管内凝固(disseminated intravascular coagulation:DIC)の治療としてに,AT活性値>70%が期待されます。私は,出血合併症を減じるために,2010年よりAT製剤は24時間持続投与で用い,ATの活性値の極端な上昇を抑え,トラフ活性値としてAT活性値>70%を目標として使用することを推奨しています。
6.急性肝不全で考える栄養療法
急性肝不全においては,アンモニアや尿素窒素が上昇しやすいために,蛋白を含む栄養制限をする傾向がありますが,低栄養状態を避けるために25 kcaL/kg/日を目標とした適切な栄養管理とできるとよいです。この際に注意する内容は,①アミノ酸バランス,②微量元素,③ビタミン,④脂質のモニタリングです。
アミノ酸補充については,1日量1.2 g/kgを最低量として維持することは,生命維持の基本と考えられています。しかし,チロシン,チロキシン,フェニルアラニン,トリプトファン,ヒスチジンの5つの芳香族アミノ酸(aromatic amino acid:AAA)や脂肪族アミノ酸のメチオニンなどの代謝は,肝機能低下状態で遅れ,アンモニアが蓄積することに注意しなければなりません。一方で,バリン,ロイシン,イソロイシンなどの分枝鎖アミノ酸(branched chain amino acid:BCAA)は,アンモニア代謝の基質となります。このため,血液中のBCCA/チロシン比(BTR)やBCAA/AAA比(Fisher比)を評価し,アミノ酸バランスを分枝鎖アミノ酸BCAAに傾ける管理となる場合があります。
このFisher比が低下している場合には,芳香族アミノ酸やメチオニンの投与量を下げるために,アミノレバン®,モリヘパミン®などの肝不全用アミノ酸製剤を使う場合もあります。芳香族アミノ酸や含硫アミノ酸を減らして Fischer 比を正常に維持できるように工夫します。臨床研究エビデンスとしてのBCAAは,2015年のCochrane Database16)においては肝性脳症の軽減には有用とされていますが,死亡率を改善するまでには至っていません。また,実臨床では,腸内細菌層の維持として乳酸菌,ビヒズス菌,カルピス菌,ラブレ菌などのプロバイオティクスを経腸投与することで,肝性脳症を軽減させようとする試みがあります。さらに,経腸栄養を最小量とし,中心静脈路より肝不全用アミノ酸製剤を併用する場合があり,いずれにしましても,消化管におけるバクテリアのアンモニア産生,肝臓での芳香族アミノ酸によるアンモニア産生に注意する一方で,どのようにアミノ酸投与を行なうかが,栄養面での鍵となります。
また,脂質代謝においては,リン脂質や総コレステロール,リン脂質,リポ蛋白が低下する可能性に注意します。総コレステロール,トリグリセリド,リポ蛋白,全脂質検査などの脂質評価を必要な時期に行い,脂質の補充を少なくとも下限領域レベルまでには適正化しなければなりません。肝不全に使用される傾向がある経腸栄養剤ヘパン®(EAファーマ株)1包 80 g中には,ダイズ油 2.80 g,トコフェロール酢酸エステル 16.6 mg,レチノール酢酸エステル 720 IU,エルゴカルシフェロール 3.8 μgです。一方で,経静脈投与として用いられているイントラリピッドやイントラリポスは,脂質モニタリングのできない環境では塞栓症や凝固障害助長のために禁忌とされています。この観点では,1%脂肪製剤として使用されているプロポフォールも原則としてしよう禁忌となります。以上には留意して対応する必要があります。
急性肝不全において経腸栄養を完成させる基盤としては,まず虚血や下血を起こさなさない呼吸・循環・凝固線溶の管理に注意し,消化管が浮腫化しないうちに早期に経腸栄養を完成させることが必要となります。その上で,①アミノ酸バランス,②亜鉛やセレンを含む適切な微量元素,③ビタミン,④脂質の補充を経腸投与できると良いです。
7.急性肝不全の治療・薬物療法
ウイルス病態では抗ウイルス薬と免疫グロブリン療法,自己免疫病態ではステロイド療法,大量免疫グロブリン療法,血漿交換法を検討します。肝臓については,ウルソデオキシコール酸(1日600 mg,1日最大量 900 mg,3分割,経管投与),グリチルリチン酸(強力ネオミノファーゲンC®:1日最大量100 mL 静注)を併用します。強力ネオミノファーゲンC®におけるDAMPs阻害作用や肝庇護剤に期待します。
8.肝移植の選択と管理
本邦における肝移植の10年生存率は70%以上です17)。他の重症疾患と比較しても良好な治療成績であり,集中治療で十分な効果が得られずに非代償性肝硬変に至った場合には,肝移植を治療の選択肢とすることが適切と思います。非代償性肝硬変では,Child-Turcotte-Pughスコア7点以上で臓器移植ネットワークの脳死肝移植待機リストに登録が可能となります。その上で,the Model for End-stage Liver Disease(MELD)スコアにおける17点以上では,肝移植待機中の死亡率が移植後の死亡率を有意に上回ることが報告されています18)。MELDスコア(メイヨークリニック計算表MELD Calculator:https://optn.transplant.hrsa.gov/resources/allocation-calculators/meld-calculator/)は,ビリルビン,プロトロンビン時間,クレアチニン,透析治療の有無で算出されるスコアであり,17点以上では肝移植を急ぐ方針となります。肝移植に向けた集中治療管理では,① 意識状態の維持(脳浮腫回避,頭蓋内出血および脳梗塞の回避),② 感染制御(血流感染予防,無気肺予防を含む),③ 出血合併症の回避,④ 腫瘍合併の否定,⑤ 筋萎縮の回避,⑥ 水・電解質管理(ナトリウムバランスなど),これらの6つを重視します。
メッセージ
急性肝不全やショック肝では,対症療法にとどまらずに,成因を評価し,成因を治療することが重要です。それを支える全身管理として,接触感染予防策の徹底,感染管理,意識,呼吸,循環,腎臓,電解質,凝固線溶,栄養,リハビリテーションなどを統合的に評価し,実践することが必要です。肝機能低下の重症病態においては,感染や虚血は,炎症誘導因子として,全身状態を複雑化したものとして悪化させることに注意しなければなりません。炎症の遷延を避け,早期から適切な栄養とリハビリテーションを目標とし,筋萎縮を避ける必要があります。本稿は,2016年度版として用意したものです。適時追記と改定を行います。急性肝炎およびショック肝の全身管理として,参考とされてください。
文 献
1. 持田 智, 滝川康裕, 中山伸朗, 他. 我が国における「急性肝不全」の概念, 診断基準の確立: 厚生労働省科学研究費補助金 (難治性疾患克服研究事業) 「難治性の肝・胆道疾患に関する調査研究」班, ワーキンググループ-1, 研究報告. 肝臓 2011; 52: 393-398.
2. 持田 智. 急性肝不全: 概念, 診断基準とわが国における実態. 日本消化器病学会雑誌 2015; 112: 813-821.
3. 第5回大山(小児肝臓)ワークショップ. 日児誌.1989;93:212-214.
4. Doğan I, Ergün M, Cindoruk M, Unal S. Acute hepatitis induced by Epstein-Barr virus infection: a case report. Turk J Gastroenterol. 2007;18:119-21.
5. Davalos F, Chaucer B, Zafar W, Salman S, Nfonoyim J. Dasatinib-Induced CMV Hepatitis in an Immunocompetent Patient: A Rare Complication of a Common Drug. Transl Oncol. 2016;9:248-50.
6. Komura T, Ohta H, Nakai R, et al. Cytomegalovirus Reactivation Induced Acute Hepatitis and Gastric Erosions in a Patient with Rheumatoid Arthritis under Treatment with an Anti-IL-6 Receptor Antibody, Tocilizumab. Intern Med. 2016;55:1923-7.
7. 厚生労働省「難治性の肝・胆道疾患に関する調査研究」班編.「自己免疫性肝炎(AIH)の診療ガイド」 文光堂,東京,2011
8. 恩地森一,銭谷幹男,山本和秀,他. 自己免疫性肝 炎の診断指針・治療指針(2013 年).肝臓 2013; 54:723-725.
9. 松井 陽.小児劇症肝炎(急性肝不全)の全国調査.「難治 性の肝・胆道疾患に関する調査研究」平成 17 年度 研究報告書.
10. Eleftheriadis T, Pissas G, Liakopoulos V, Stefanidis I. Cytochrome c as a Potentially Clinical Useful Marker of Mitochondrial and Cellular Damage. Front Immunol. 2016;7:279.
11. Shi Q, Yang X, Mattes WB, et al. Circulating mitochondrial biomarkers for drug-induced liver injury. Biomark Med. 2015;9:1215-23.
12. Wenceslau CF, McCarthy CG, Szasz T, et al. Mitochondrial damage-associated molecular patterns and vascular function. Eur Heart J. 2014;35:1172-7.
13. Kellum JA, Lameire N; KDIGO AKI Guideline Work Group. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17:204.
14. Lameire N, Kellum JA; KDIGO AKI Guideline Work Group. Contrast-induced acute kidney injury and renal support for acute kidney injury: a KDIGO summary (Part 2). Crit Care. 2013;17:205.
15. Mori H, Hiraoka K, Yorifuji R, et al. Adsorption of human recombinant erythropoietin on dialysis membranes in vitro. Artif Organs. 1994;18:725-8.
16. Gluud LL, Dam G, Les I, et al. Branched-chain amino acids for people with hepatic encephalopathy. Cochrane Database Syst Rev. 2015 :CD001939.
17. 市田隆文,玄田拓哉,平野克治. わが国における脳死肝移植医療の現状と問題点. 肝臓 2015;56:79-87.
18. Merion RM, Schaubel DE, Dykstra DM, et al. The survival benefit of liver transplantation. Am J Transplant. 2005;5:307-13.
表と図
表1 急性肝不全の定義と分類

表2 成人肝性脳症に対する犬山分類

表3 小児肝性脳症の分類

表4 急性肝不全における発症要因の評価

表5 自己免疫性肝炎の診断指針・治療指針

表6 急性腎傷害 KDIGOクライテリア

参照 メイヨークリニック計算表MELD Calculator
the Model for End-stage Liver Disease(MELD)スコアにおける17点以上では,肝移植待機中の死亡率が移植後の死亡率を有意に上回ることが報告されています。