Kyoto University Newsletter Raku-Yu
Global Transformation of Emergency and Critical Care Medicine in Kyoto University
Naoyuki Matsuda MD, PhD
Associate Professor
Department of Primary Care & Emergency Medicine, Kyoto University
Profile Introduction
Associate Prof. Matsuda, born the grandson of a surgeon and the son of a pediatrician, at first wanted to become a physician himself. However, after entering Hokkaido University, his interests were broadened and he chose to specialize in anesthesiology from which he could view a wide variety of specialties, and then leapfrogged into the world of emergency medicine and critical care medicine. When emergency medical treatment became a specialty on a nationwide scale he took an active part in its establishment as a member of the emergency department ward in Hokkaido University Hospital. He moved to Kyoto University in 2007, and he has been working tirelessly to cultivate emergency medical specialists and to ascertain an emergency health care system both for the University Hospital and the local communities. When he moved to Kyoto for his present post, those around him worried that Kyoto was behind the times as it was slower to establish emergency medical systems than other prefectures, but he now states brightly, “The academic research environment of Kyoto University is preeminent and the potential of doctors and individual students is also excellent. I’m very glad I came here because it was, above all, a pleasure to construct things from scratch.”As for the present conditions of emergency medicine, Associate Prof. Matsuda strongly feels the necessity for cultivating the ability to diagnose the condition of the individual patient first and foremost, even going so far as to consider his or her life background. “Nowadays, it seems that the specialization of diagnosis in each department has advanced to the point that patients are provided a diagnosis which equals the name of a disease, and a uniform medical treatment is prescribed. However, even with the same disease, symptoms are manifested differently depending on the individual.” After saying this, he continued with this interesting statement, “One of the merits of medical treatment in Japan is that it originally intended to seek‘medical care with hospitality (Motenashi-no-Iryo),’ which means that each patient should be carefully diagnosed and the best treatment should be found for patients respectively.”Associate Prof. Matsuda’s logical and intelligible words delivered with a smile as he continues to listen carefully toothers, resounds with a significant persuasive power.


Essay
Kyoto was previously known as the most underdeveloped region regarding emergency medicine in Japan. The Department of Primary Care & Emergency Medicine was established at Kyoto University in April 2006. At present, specialists in emergency and intensive care medicine representing all of Japan have begun to gather in Kyoto, and to steadily improve the clinical outcome of emergency care. Our department is dedicated to providing sufficient acute disease treatment to university staff, our students, and neighboring patients, and is projected to improve the quality of emergency and intensive care medicine not only in Kyoto but throughout Japan.
All faculty members and students of Kyoto University share the mentality to aspire to be “the best” and to lead the world in their specialties. Aside from being encouraged by words such as “Boys, be ambitious”*, each person has his/her unique academic goal and wishes to contribute to the world through their achievements. Despite such an environment, emergency and intensive care medicine has remained a lagging field of science, failing to show the world sufficient academic accomplishments. This situation derives from the lack of philosophy or a simplified hypothesis concerning the aims of emergency and intensive care medicine. Emergency medicine requires a medical system to appropriately assess the urgency of the condition and promptly initiate treatment on the one hand, and the ability to assiduously analyze acute disorder conditions on the other.
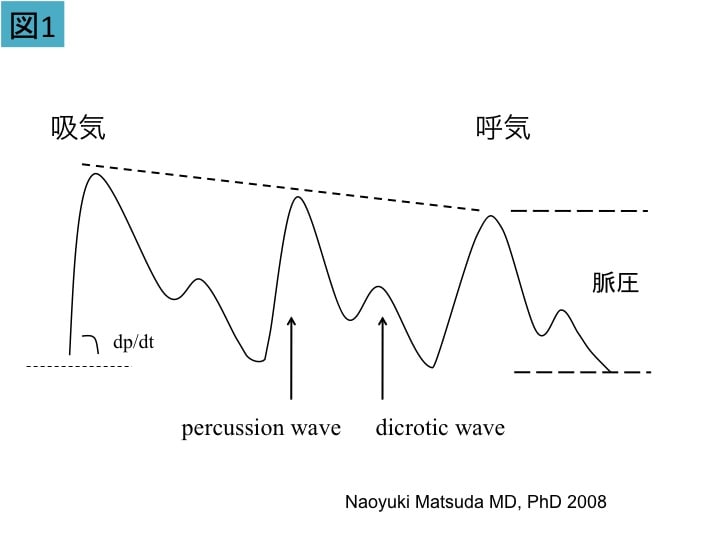
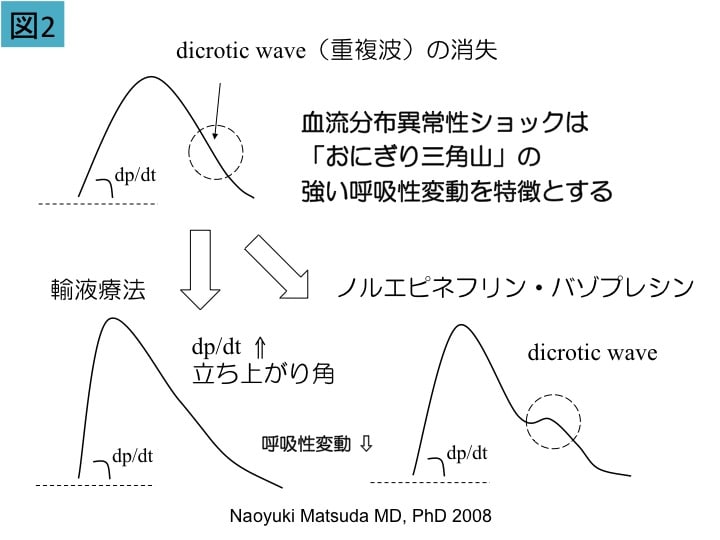
Presently, I am conducting research on the pathophysiology and therapeutics of systemic inflammatory response syndrome. Vascular endothelial cell injury associated with this syndrome is the pathological condition to which emergency and critical care medicine attaches the greatest importance. In addition, a medical system that can completely cure conditions including multiple traumas, multiple organ failure, and post-resuscitation encephalopathy is necessary. For example, even pulmonary contusion after a traffic accident is not serious if it heals quickly, as in children. Influenza is also of low-level concern if it takes a mild course by immunological enhancement. The promotion of injury healing and enhancement of immunological competence are other aims of emergency medicine. I deem that the establishment of a discipline that enables physicians to avoid panicking or to restore composure is necessary.
The breeze blows gently in Kyoto. The Kamo River flowing like a kimono emanates the sounds of running water and musical instruments. One reason for the sophisticated atmosphere here is that the Kyoto dialect has softer voiced consonants. I always emphasize four things to young doctors and young researchers: (1) Never say “No”, (2) Step lively, (3) Remember to smile, (4) Greet all in a loud, clear voice. The adoption of these measures creates a revitalized atmosphere in our university and laboratory. Their performance must not become introverted, inactive, and sullen-faced. Science begins by simplifying individual, habitual concepts, and then embracing a wide range of aspects. We wish to revere the quiet atmosphere of Kyoto, always seek a complexity-free emergency care system, and enrich the science of acute period pathophysiology through many academic accomplishments. I hope to disseminate this new discipline of emergency and intensive care medicine from Kyoto throughout the world.
* The famous phrase attributed to William Smith Clarke, the first vice president of Sapporo Agricultural College, which later became part of Hokkaido University in Japan.