Acid-base problems in diabetic ketoacidosis.
Kamel KS, Halperin ML.
N Engl J Med. 2015;372:546-54.
<松田直之 コメント>
我々の救急・集中治療部にも,年間で4例程度の重症な糖尿病性ケトアシドーシスの搬入があります。
とても良く記載されている素晴らしい総説です。
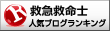
This review focuses on three issues facing clinicians who care for patients with diabetic ketoacidosis; all of the issues are related to acid–base disorders. The first issue is the use of the plasma anion gap and the calculation of the ratio of the change in this gap to the change in the concentration of plasma bicarbonate in these patients; the second concerns the administration of sodium bicarbonate; and the third is the possible contribution of intracellular acidosis to the development of cerebral edema, particularly in children with diabetic ketoacidosis. In this article, we examine the available data and attempt to integrate the data with principles of physiology and metabolic regulation and provide clinical guidance.



強い要望により,学術面のみの再開とします。
2015年3月27日 松田直之
Kamel KS, Halperin ML.
N Engl J Med. 2015;372:546-54.
<松田直之 コメント>
我々の救急・集中治療部にも,年間で4例程度の重症な糖尿病性ケトアシドーシスの搬入があります。
とても良く記載されている素晴らしい総説です。
This review focuses on three issues facing clinicians who care for patients with diabetic ketoacidosis; all of the issues are related to acid–base disorders. The first issue is the use of the plasma anion gap and the calculation of the ratio of the change in this gap to the change in the concentration of plasma bicarbonate in these patients; the second concerns the administration of sodium bicarbonate; and the third is the possible contribution of intracellular acidosis to the development of cerebral edema, particularly in children with diabetic ketoacidosis. In this article, we examine the available data and attempt to integrate the data with principles of physiology and metabolic regulation and provide clinical guidance.
強い要望により,学術面のみの再開とします。
2015年3月27日 松田直之