








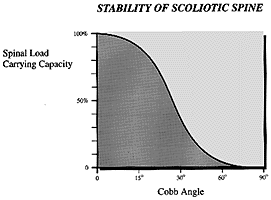
(添付図は、イリノイ工科大学航空機械工学 Patwardhan博士の研究より)
特発性側弯症の治療方針として必ず登場するのが、
◇軽度側弯(30°未満)定期的に経過観察、進行を見逃さない
◇中等度側弯(30°~50°)装具による矯正治療
◇高度側弯(50°以上、胸腰椎側弯・腰椎側弯の場合は40°以上)手術療法必要
(日本側彎症学会Q&Aより引用)
という説明です。
私はこれを先生がたの長年の治療結果から生み出された経験則にもとづく方針と
ばかり思い込んでいました。
もちろん、長年の治療によって蓄積されたデータに裏付けられているわけですが、
この方針をサポートする科学文献が1986年、1987年に発表されていたことを知り
ましたので、ご紹介したいと思います。
添付図は、この研究を発表されたPatwardhan博士のコンピューター解析図です。
このPatwardhan博士は医師ではなく、航空工学を専門とする先生で、この研究は
特発性側弯症をバイオメカニクス(生体医用工学)の面から、コンピューター分析
しています。人間の身体を工学的学問、知識を用いて分析するのが、バイオメカニクス
といわれる分野です。例えば、先の「夢の扉」で東京大学の工学部の教授が義手を
作製する上でも、基本になっているのは、バイオメカニクスです。いわば、医学
知識と工学知識とが融合した学問とイメージしていただければよいと思います。
ヒトは二本足で立って歩行する動物です。そのとき「立つ」という動作を可能に
している脊柱(せぼね)に、どういう力(これを荷重/かじゅうと言います)が働いて
いるのか、ということを特発性側弯症との関係でコンピューター分析した研究が
下記に記載した2本の文献です。
この図を用いて簡略した説明をさせていただきますと、
脊柱が軽くカーブした段階では、ヒトの身体には、そのカーブを「支える」能力
が残っています。(骨格自体の力や筋力の力と考えるとわかりやすいと思います)
しかし、このカーブが次第に大きくなって、ある限界を超えると、もうヒトには
その曲がった脊柱を元に戻す力はなくなり、どんどんと悪くなっていくばかりです
15度(~20度)であれば、元にもどる力、あるいは戻らなくても、そのカーブがそれ
以上は悪くならないだけの力を身体は持っています。
20度(~25度)を超えると、カーブを支える力は減少し、どんどんとカーブが大きく
なります。ここで曲がる力に抵抗を加えようとするのが、「装具」という事です
装具をしなければ、カーブは悪くなりばかりだからです。
50度を越えると、装具でも支えきれなくなります。
.............................................................
バイオメカニクスの分析によって、人体と「荷重」の関係、あるいはカーブと
それを支えようとする人体の力との相関関係が、「科学」という面から裏づけ
されたことになります。
それは、まさに特発性側弯症の治療に長年にわたって携わってきた整形外科の先生
がたの経験とも合致するものでした。
思春期のこどもたちの中に、「ある角度」を超えるこどもがいる。そのこども達に
はすぐに装具療法をしなければならない。
そして、その装具療法中のこども達の中にも、さらに急激に進行するこどもと
進行しない/進行が止められるこどもがいることを先生たちは知っていました。
これは一種のアルゴリズムなのですが、そのアルゴリズムを図式化して示した
ものが、添付図となります。
---------------------------------------------------------------------
Dr.Pawardhan等はコブ角0度~60度でのコンピューターモデルを作成し検証した。
このモデルによってもなぜ医師が15度~20度のこどもに装具療法を開始しないかを
説明することができる。15度~20度のカーブは進行することがなく、そして25度以
上になるとカーブは進行することから、医師は装具療法を開始する、ということの
説明ができるのである。そしてこのコンピューターモデルからは、装具をしている
にも係わらず、なぜ45度を越えるとさらにカーブが進むのか、50度を超えると大人
になってもカーブが進むのもかも説明することができる。
Dr. Patwardhan and his engineering colleagues did a theoretical computer
modeling study on curves from 0o-60o that shows that the larger a curve
is, the more likely it is to progress6 (figure 9). These modeling studies
help to explain why we don't treat children with 15o and 20o spinal
curves as they are not all going to progress and why we do begin orthotic
treatment for children with progressive curves that are over 25o. This
also helps to explain why children with curves over 45o are likely to
progress even if they are braced and why someone with a spinal curve over
50o is likely to progress even as an adult.
専門誌 Spine. 1987 Jul-Aug;12(6)
Progression of unsupported curves in adolescent idiopathic scoliosis.
Department of Mechanical and Aerospace Engineering, Illinois Institute of
Technology, Chicago.
Stability of three types of double scoliotic curves of 10-40 degrees was
analyzed using a biomechanical model: double primary (Type I), primary
thoracic with compensatory lumbar (Type II), and primary lumbar with
compensatory thoracic (Type III). The load-carrying capacity of each
curve was analyzed as a function of magnitude of the curve, its location
and flexibility. Curve magnitude was found to be the most influential
parameter governing the stability of a scoliotic curve up to 30 degrees.
Results suggest that in evaluating curves of comparable magnitudes, Type
I and II curves are more likely to progress and, therefore, should be
braced at an earlier stage than Type III curves.
専門誌 J Biomech. 1986;19(2):
A biomechanical analog of curve progression and orthotic stabilization in
idiopathic scoliosis.
A biomechanical analog of curve progression and orthotic stabilization in
idiopathic scoliosis has been developed using the classical theory of
curved beam-columns. The interaction of the spinal musculature and other
supporting structures is incorporated in the model using an equivalent
flexural rigidity. The stability of a given scoliotic curve relative to a
normal spine is described in terms of the so-called critical load ratio
(Pc/Pe). This dimensionless quantity appears in the exact solution of the
governing differential equation and boundary conditions. It is defined as
the ratio of the load bearing capacity of a scoliotic spine (Pc) to that
of a normal spine where the load bearing capacity of a normal spine is
defined as Euler's buckling load (Pe). The computation of Pc/Pe is based
upon a maximum allowable moment criterion. This model is used to study
the effect of the degree of initial curvature and curve pattern in the
frontal plane on the stability of untreated idiopathic scoliosis.
Although restricted to two-dimensions, the model appears to demonstrate
the synergistic effects of end support, transverse loading, and curve
correction on improvement in relative stability of an orthotically
supported scoliotic curve. The results of this study are in qualitative
agreement with clinical findings that are based on long-term studies of
natural history of idiopathic scoliosis and of patients undergoing
orthotic management for scoliosis.
特発性側弯症の治療方針として必ず登場するのが、
◇軽度側弯(30°未満)定期的に経過観察、進行を見逃さない
◇中等度側弯(30°~50°)装具による矯正治療
◇高度側弯(50°以上、胸腰椎側弯・腰椎側弯の場合は40°以上)手術療法必要
(日本側彎症学会Q&Aより引用)
という説明です。
私はこれを先生がたの長年の治療結果から生み出された経験則にもとづく方針と
ばかり思い込んでいました。
もちろん、長年の治療によって蓄積されたデータに裏付けられているわけですが、
この方針をサポートする科学文献が1986年、1987年に発表されていたことを知り
ましたので、ご紹介したいと思います。
添付図は、この研究を発表されたPatwardhan博士のコンピューター解析図です。
このPatwardhan博士は医師ではなく、航空工学を専門とする先生で、この研究は
特発性側弯症をバイオメカニクス(生体医用工学)の面から、コンピューター分析
しています。人間の身体を工学的学問、知識を用いて分析するのが、バイオメカニクス
といわれる分野です。例えば、先の「夢の扉」で東京大学の工学部の教授が義手を
作製する上でも、基本になっているのは、バイオメカニクスです。いわば、医学
知識と工学知識とが融合した学問とイメージしていただければよいと思います。
ヒトは二本足で立って歩行する動物です。そのとき「立つ」という動作を可能に
している脊柱(せぼね)に、どういう力(これを荷重/かじゅうと言います)が働いて
いるのか、ということを特発性側弯症との関係でコンピューター分析した研究が
下記に記載した2本の文献です。
この図を用いて簡略した説明をさせていただきますと、
脊柱が軽くカーブした段階では、ヒトの身体には、そのカーブを「支える」能力
が残っています。(骨格自体の力や筋力の力と考えるとわかりやすいと思います)
しかし、このカーブが次第に大きくなって、ある限界を超えると、もうヒトには
その曲がった脊柱を元に戻す力はなくなり、どんどんと悪くなっていくばかりです
15度(~20度)であれば、元にもどる力、あるいは戻らなくても、そのカーブがそれ
以上は悪くならないだけの力を身体は持っています。
20度(~25度)を超えると、カーブを支える力は減少し、どんどんとカーブが大きく
なります。ここで曲がる力に抵抗を加えようとするのが、「装具」という事です
装具をしなければ、カーブは悪くなりばかりだからです。
50度を越えると、装具でも支えきれなくなります。
.............................................................
バイオメカニクスの分析によって、人体と「荷重」の関係、あるいはカーブと
それを支えようとする人体の力との相関関係が、「科学」という面から裏づけ
されたことになります。
それは、まさに特発性側弯症の治療に長年にわたって携わってきた整形外科の先生
がたの経験とも合致するものでした。
思春期のこどもたちの中に、「ある角度」を超えるこどもがいる。そのこども達に
はすぐに装具療法をしなければならない。
そして、その装具療法中のこども達の中にも、さらに急激に進行するこどもと
進行しない/進行が止められるこどもがいることを先生たちは知っていました。
これは一種のアルゴリズムなのですが、そのアルゴリズムを図式化して示した
ものが、添付図となります。
---------------------------------------------------------------------
Dr.Pawardhan等はコブ角0度~60度でのコンピューターモデルを作成し検証した。
このモデルによってもなぜ医師が15度~20度のこどもに装具療法を開始しないかを
説明することができる。15度~20度のカーブは進行することがなく、そして25度以
上になるとカーブは進行することから、医師は装具療法を開始する、ということの
説明ができるのである。そしてこのコンピューターモデルからは、装具をしている
にも係わらず、なぜ45度を越えるとさらにカーブが進むのか、50度を超えると大人
になってもカーブが進むのもかも説明することができる。
Dr. Patwardhan and his engineering colleagues did a theoretical computer
modeling study on curves from 0o-60o that shows that the larger a curve
is, the more likely it is to progress6 (figure 9). These modeling studies
help to explain why we don't treat children with 15o and 20o spinal
curves as they are not all going to progress and why we do begin orthotic
treatment for children with progressive curves that are over 25o. This
also helps to explain why children with curves over 45o are likely to
progress even if they are braced and why someone with a spinal curve over
50o is likely to progress even as an adult.
専門誌 Spine. 1987 Jul-Aug;12(6)
Progression of unsupported curves in adolescent idiopathic scoliosis.
Department of Mechanical and Aerospace Engineering, Illinois Institute of
Technology, Chicago.
Stability of three types of double scoliotic curves of 10-40 degrees was
analyzed using a biomechanical model: double primary (Type I), primary
thoracic with compensatory lumbar (Type II), and primary lumbar with
compensatory thoracic (Type III). The load-carrying capacity of each
curve was analyzed as a function of magnitude of the curve, its location
and flexibility. Curve magnitude was found to be the most influential
parameter governing the stability of a scoliotic curve up to 30 degrees.
Results suggest that in evaluating curves of comparable magnitudes, Type
I and II curves are more likely to progress and, therefore, should be
braced at an earlier stage than Type III curves.
専門誌 J Biomech. 1986;19(2):
A biomechanical analog of curve progression and orthotic stabilization in
idiopathic scoliosis.
A biomechanical analog of curve progression and orthotic stabilization in
idiopathic scoliosis has been developed using the classical theory of
curved beam-columns. The interaction of the spinal musculature and other
supporting structures is incorporated in the model using an equivalent
flexural rigidity. The stability of a given scoliotic curve relative to a
normal spine is described in terms of the so-called critical load ratio
(Pc/Pe). This dimensionless quantity appears in the exact solution of the
governing differential equation and boundary conditions. It is defined as
the ratio of the load bearing capacity of a scoliotic spine (Pc) to that
of a normal spine where the load bearing capacity of a normal spine is
defined as Euler's buckling load (Pe). The computation of Pc/Pe is based
upon a maximum allowable moment criterion. This model is used to study
the effect of the degree of initial curvature and curve pattern in the
frontal plane on the stability of untreated idiopathic scoliosis.
Although restricted to two-dimensions, the model appears to demonstrate
the synergistic effects of end support, transverse loading, and curve
correction on improvement in relative stability of an orthotically
supported scoliotic curve. The results of this study are in qualitative
agreement with clinical findings that are based on long-term studies of
natural history of idiopathic scoliosis and of patients undergoing
orthotic management for scoliosis.
















