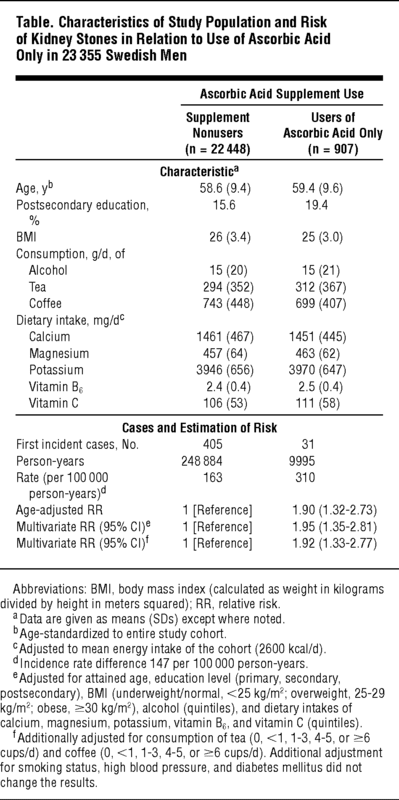
表 2万3355人のスウェーデン人男性におけるアスコルビン酸使用に関連する試験集団の特性と腎結石のリスク
No.1 2020/05/15改訂 アスコルビン酸と腎臓結石に関連はない 前向き研究の解釈と対策1
2020/05/15改訂 赤字の部分を追加しました
調査・評価の結論
(1)このブログ記事で述べている論文「男性のアスコルビン酸サプリメントと腎臓結石の発生率:前向き研究」は、研究方法に問題があり、信頼性が低いため、この論文の結果は使用できません。
よって、男性・女性、全年齢で、細菌・ウイルス感染の対処に、高投与量のアスコルビン酸が腎臓結石を起こすという証拠はなく、使用可能です。
*この論文に対しては、「オーソモレキュラー医学ニュースサービスー日本語版」の批判・否定記事があり、オーソモレキュラー医学の専門家もアスコルビン酸による腎臓結石を否定しています。
「2013-04-01ビタミンCは腎臓結石の原因ではない!(反対にビタミンCは腎臓結石のリスクを減らしている)」
https://isom-japan.org/news/detail?uid=yd4GT1548853962
(2) 感染症にビタミンCを使用する時、アスコルビン酸が分解して生じるシュウ酸が生成するシュウ酸カルシウム結晶による腎結石の発生は、絶対にないかと問われたら、誰もゼロであるという根拠を出せないと思います。
ゼロではないならば、それに対してどのような防御策があるかが、現実的な問題です。
感染症にビタミンCを使用して、シュウ酸結石を予防するなら、クエン酸(レモン水、クエン酸、クエン酸ナトリウム)を使用する、そして必要と考えるならば重曹、マグネシウム(サプリメント)、フィチン酸(有機栽培米ぬか)を併用する方法があります。
(3)アスコルビン酸の安全性に関しては、次の総説に安全であることを示すまとめがあります。
ブログ記事の全訳
ビタミンCの安全性: 都市伝説Safety of Vitamin C: Urban Legends
https://blog.goo.ne.jp/gadamski/e/e66906656bac689c0cb59cc27db77a1a
University of Helsinki, Helsinki, Finlandヘルシンキ大学、ヘルシンキ、フィンランド、Department of Public Health公衆衛生学部
Harri Hemilä (ビタミンC研究の専門家)の調査結果です
++++++++++++++++++++++++++++++++++++++++++++++
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1568519#ild120089t1
Research Letter研究レター
Mar 11, 2013、2013年3月11日
Ascorbic Acid Supplements and Kidney Stone Incidence Among Men: A Prospective Study
男性のアスコルビン酸サプリメントと腎臓結石の発生率:前向き研究
Laura D. K. Thomas, MSc; Carl-Gustaf Elinder, MD; Hans-Göran Tiselius, MD; et alAlicja Wolk, DrMedSc; Agneta Åkesson, PhD
Author Affiliations Article Information
JAMA Intern Med. 2013;173(5):386-388. doi:10.1001/jamainternmed.2013.2296
Urinary oxalate is an important determinant of calcium oxalate kidney stone formation.1
尿中シュウ酸塩は、シュウ酸カルシウム腎結石形成の重要な決定因子です。1
Vitamin C is excreted in urine both in its unmetabolized form and as oxalate; however, there remains considerable uncertainty over the kidney stone risk that may be associated with ascorbic acid supplement use.2
ビタミンCは代謝されていない形とシュウ酸塩として尿中に排泄されます。 しかし、アスコルビン酸サプリメントの使用に関連する可能性のある腎臓結石のリスクについては、かなりの不確実性が残っています。2
We examined whether ascorbic acid supplements (approximately 1000 mg) were associated with kidney stones in a population-based, prospective cohort of men.
アスコルビン酸サプリメント(約1000 mg)が人口ベースの男性の前向きコホートで腎臓結石と関連しているかどうかを調べました。
Methods方法
The Cohort of Swedish Men (COSM) has been described elsewhere.3
スウェーデン男性のコホート(COSM)は他の場所で説明されています。
In brief, 48 850 men, aged 45 to 79 years at baseline, were recruited in 1997 (response rate, 49%).
手短に言えば、ベースラインで45〜79歳の48 850人の男性が1997年に採用されました(回答率49%)。
Detailed diet and lifestyle data were collected at baseline using a self-administered questionnaire.
自己管理質問票を使用して、詳細な食事およびライフスタイルデータをベースライン時に収集しました。
Based on validated questions, men reported their use of ascorbic acid (sensitivity = 67% and specificity = 93%)4 and of 20 other supplement types.
検証済みの質問に基づいて、男性はアスコルビン酸(感度= 67%、特異度= 93%)4と他の20種類のサプリメントの使用を報告しました。
We excluded those with incorrect national registration numbers, implausible energy intake, prebaseline cancer diagnosis, and missing supplement use data and those diagnosed as having kidney stones prior to baseline, based on registry (n = 1612) and self-reported (n = 5898) data, because these men may have changed their diet or supplement use based on medical advice.
レジストリ(n = 1612)と自己申告(n = 5898)に基づいて、不正確な国内登録番号、信じられないほどのエネルギー摂取量、ベースライン前の癌診断、およびサプリメント使用データの欠落があるものと、ベースラインより前に腎結石があると診断されたものを除外しました これらの男性は、医学的アドバイスに基づいて食事やサプリメントの使用を変更した可能性があるためです。
We also excluded users of supplements other than ascorbic acid as this may be a significant source of confounding (n = 12 873).
アスコルビン酸以外のサプリメントの使用も除外しました。これは交絡の重要な原因となる可能性があるためです(n = 12 873)。
For comparison, we repeated the analysis for multivitamin (only) users.
比較のために、マルチビタミン(のみ)ユーザーの分析を繰り返しました。
First incident cases of kidney stones (International Statistical Classification of Diseases, 10th Revision code N20) were ascertained from January 1, 1998, to December 31, 2009, using registry data.
腎臓結石の最初の発症症例(国際疾病統計分類、第10改訂コードN20)は、登録データを使用して、1998年1月1日から2009年12月31日まで確認されました。
We estimated hazard ratios (hereafter, relative risks [RRs]) with Cox proportional hazards regression models using attained age as the timescale.
到達年齢をタイムスケールとして使用して、Cox比例ハザード回帰モデルでハザード比(以下、相対リスク[RR])を推定しました。
Follow-up was censored at date of kidney stone diagnosis, death, or end of follow-up, whichever occurred first.
フォローアップは、腎結石の診断、死亡、またはフォローアップの終了のいずれか早い方の日に行われた。
The Schoenfeld residual test indicated no violation of the proportional hazard assumption.
シェーンフェルド残差検定は、比例ハザードの仮定に違反していないことを示しました。
Dose-response was assessed using the frequency-of-use data, which were available for 91.5% of ascorbic acid users.
用量反応は、アスコルビン酸ユーザーの91.5%が利用できた使用頻度データを使用して評価されました。
The linear trend across categories was tested using the median tablet usage within each group as a continuous variable.
カテゴリ間の線形傾向は、連続変数として各グループ内の中央値の錠剤の使用量を使用してテストされました。
Ethical approval was granted by the regional ethical review board in Stockholm, Sweden, and return of the completed questionnaire was considered to imply informed consent.
スウェーデンのストックホルムにある地域の倫理審査委員会によって倫理的な承認が与えられ、記入済みのアンケートの返却は、インフォームドコンセントを意味すると見なされました。
Results結果
During 11 years of follow-up we ascertained 436 first incident cases of kidney stones.
11年間のフォローアップ中に、腎結石の最初の発症436件を確認しました。
(訳注: ベースラインで45〜79歳を11年間追跡すると、56~90歳まで追跡することになる)
Ascorbic acid use was associated with a statistically significant 2-fold increased risk (Table).
アスコルビン酸の使用は、統計的に有意な2倍のリスク増加と関連していた(表)。
In contrast, multivitamin use was not associated with kidney stone risk (RR, 0.86 [95% CI, 0.62-1.19]).
対照的に、マルチビタミンの使用は腎臓結石のリスクとは関連していませんでした(RR、0.86 [95%CI、0.62-1.19])。
Users of only ascorbic acid taking fewer than 7 (median) and 7 or more tablets per week showed increased risks of RR, 1.66 (95% CI, 0.99-2.79) and RR, 2.23 (95% CI, 1.28-3.88), respectively, compared with supplement nonusers in the full multivariate-adjusted model (P value for trend = .001).
週に7(中央値)未満および7以上の錠剤を服用しているアスコルビン酸のみのユーザーは、それぞれRR、1.66(95%CI、0.99-2.79)およびRR、2.23(95%CI、1.28-3.88)のリスクの増加を示しました 、完全な多変量調整モデルでのサプリメント非ユーザーと比較(傾向のP値= .001)。
表 23355人のスウェーデン人男性におけるアスコルビン酸使用に関連する試験集団の特性と腎結石のリスク
(冒頭の図を参照)
Commentコメント
The strengths of this study include the large population-based prospective cohort design, validated exposure data, and virtually complete follow-up of the study population through linkage to high-quality registers.
この研究の長所には、大規模な人口ベースの前向きコホート設計、検証済みの暴露データ、および高品質のレジスターとのリンクによる研究人口の事実上完全なフォローアップが含まれます。
Furthermore, analysis of kidney stone material collected from 3176 men, treated with extracorporeal shockwave lithotripsy in Stockholm County, found calcium oxalate to be the dominant component in 92.6% (H.-G.T., unpublished data).
さらに、ストックホルム郡で体外衝撃波砕石術で治療された3176人の男性から収集された腎臓結石材料の分析では、92.6%でシュウ酸カルシウムが主要成分であることがわかりました(H.-G.T.、未発表データ)。
It could thus be assumed that at least 90% of the kidney stones in our study population were composed primarily of calcium oxalate.5
したがって、私たちの研究対象集団の腎臓結石の少なくとも90%が主にシュウ酸カルシウムで構成されていると推定できます。5
Our results may not be generalizable to women, who typically have a much lower kidney stone risk.
私たちの結果は、一般的に腎結石のリスクがはるかに低い女性には一般化できない可能性があります。
Because the risk associated with ascorbic acid may depend both on the dose and on the combination of nutrients with which the ascorbic acid is ingested, our findings should not be translated to dietary vitamin C.
アスコルビン酸に関連するリスクは、アスコルビン酸の摂取量と栄養素の組み合わせの両方に依存する可能性があるため、調査結果を食事性ビタミンCに変換しないでください。
Data on the brand of supplement used were not available, and we were not, therefore, able to fully characterize the dose taken.
使用したサプリメントのブランドに関するデータは入手できなかったため、摂取した用量を完全に特徴付けることはできませんでした。
However, previous studies have demonstrated that ascorbic acid preparations available on the Swedish market typically contain 1000 mg of ascorbic acid per tablet.6
しかし、以前の研究では、スウェーデンの市場で入手可能なアスコルビン酸製剤には、通常、1錠あたりアスコルビン酸1000 mgが含まれていることが示されています6。
Supplement users may be more health conscious and therefore more likely to seek medical help; however, given the severe pain associated with kidney stones, this is unlikely to explain our findings.
サプリメントのユーザーは健康志向が強いため、医療支援を求める可能性が高くなります。 しかし、腎臓結石に伴う激しい痛みを考えると、これは私たちの発見を説明する可能性は低いです。
It is also not supported by our null results for multivitamin use.
また、マルチビタミン使用に関するnull(ゼロ)結果ではサポートされていません。
We cannot rule out the possibility of residual confounding.
交絡が残っている可能性を排除することはできません。
The rate difference was 147 of 100 000 for first incident cases; however, the recurrent nature of kidney stones implies that the absolute risk increase, for this modifiable risk factor, is potentially higher.
最初の発症症例では、レートの差は10万分の147でした。ただし、腎臓結石の再発性は、この変更可能なリスク要因の絶対的なリスクの増加が潜在的に高いことを意味します。
訳注:ビタミンCサプリメント使用者と非使用者の2群間の比較で、0.163%から0.310%へ、0.147%の腎結石の発生率の増加、表を参照)
Our findings need to be confirmed by other studies but may have important implications for the clinical advice given to kidney stone formers.
私たちの発見は他の研究によって確認される必要がありますが、腎臓結石形成者に与えられる臨床的アドバイスに重要な影響を与えるかもしれません。
Currently there are no well-documented benefits of high-dose ascorbic acid supplement use,7 and, therefore, it seems prudent to advise that high-dose preparations be avoided, particularly by those with a history of kidney stones.
現在、高用量のアスコルビン酸サプリメントの使用について十分に証明された利点はありません7。そのため、特に腎臓結石の病歴がある人は、高用量の製剤を避けるようにアドバイスするのが賢明です。
In conclusion, our results indicate that high-dose ascorbic acid supplements—one of the most commonly used vitamin preparations—are associated with a dose-dependent 2-fold increased risk of kidney stone formation among men.
結論として、我々の結果は、最も一般的に使用されているビタミン剤の1つである高用量のアスコルビン酸サプリメントが、用量依存性の男性の腎臓結石形成の2倍の増加リスクと関連していることを示しています。
Article Information
Correspondence: Dr Åkesson, Division of Nutritional Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, PO Box 210, 171 77 Stockholm, Sweden (Agneta.Akesson@ki.se).
Published Online: February 4, 2013. doi:10.1001/jamainternmed.2013.2296
Author Contributions: Dr Thomas and Åkesson had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Thomas, Wolk, and Åkesson. Acquisition of data: Wolk. Analysis and interpretation of data: Thomas, Elinder, Tiselius, Wolk, and Åkesson. Drafting of the manuscript: Thomas and Åkesson. Critical revision of the manuscript for important intellectual content: Thomas, Elinder, Tiselius, Wolk, and Åkesson. Statistical analysis: Thomas. Obtained funding: Wolk and Åkesson. Administrative, technical, and material support: Tiselius and Wolk. Study supervision: Elinder and Åkesson.
Conflict of Interest Disclosures: None reported.利益相反開示: 報告なし
Funding/Support: The research was funded by the Swedish Research Council/Research Infrastructures (grant No. 2008-5947) and Karolinska Institutet KID funding (PhD funding awarded to Ms Thomas).
資金/サポート:研究は、スウェーデン研究評議会/研究インフラストラクチャ(付与番号2008-5947)とKarolinska Institutet KIDの資金(PhD資金はMs Thomasに授与されました)によって資金提供されました。
Role of the Sponsors: The funders had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript.
Previous Presentation: This study was presented as a conference poster, “Vitamin C Supplementation and Kidney Stone Incidence Among Men: A Population-Based Prospective Cohort Study,” at the International Conference on Diet and Activity Methods, Food and Organisation; May 15, 2012; Rome, Italy.
References
1.Curhan GC, Willett WC, Speizer FE, Stampfer MJ. Twenty-four-hour urine chemistries and the risk of kidney stones among women and men. Kidney Int. 2001;59(6):2290-229811380833PubMedGoogle Scholar
2.Taylor EN, Stampfer MJ, Curhan GC. Dietary factors and the risk of incident kidney stones in men: new insights after 14 years of follow-up. J Am Soc Nephrol. 2004;15(12):3225-323215579526PubMedGoogle ScholarCrossref
3.Messerer M, Håkansson N, Wolk A, Akesson A. Dietary supplement use and mortality in a cohort of Swedish men. Br J Nutr. 2008;99(3):626-63117764599PubMedGoogle ScholarCrossref
4.Messerer M, Wolk A. Sensitivity and specificity of self-reported use of dietary supplements. Eur J Clin Nutr. 2004;58(12):1669-167115226758PubMedGoogle ScholarCrossref
5.Tiselius H. Solution chemistry of supersaturation. In: Coe FLFM, Pak CYC, Parks JH, Preminger GM, eds. Kidney Stones, Medical and Surgical Management. Philadelphia, PA: Lippincott-Raven Publishers; 1996:33-64
6.Messerer M, Johansson SE, Wolk A. The validity of questionnaire-based micronutrient intake estimates is increased by including dietary supplement use in Swedish men. J Nutr. 2004;134(7):1800-180515226472PubMedGoogle Scholar
7.Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Cochrane Database Syst Rev. 2012;3:CD00717622419320PubMedGoogle Scholar
+++++++++++++++++++++++++++++++++++++++++
スウェーデン男性のコホート(COSM)は他の場所で説明されています。3
3.Messerer M, Håkansson N, Wolk A, Akesson A. Dietary supplement use and mortality in a cohort of Swedish men. Br J Nutr. 2008;99(3):626-63117764599PubMedGoogle ScholarCrossref
論文全文
ビタミンCの摂取群の男性の詳細は、この文献にはないため不明。
よって、バイアス・偏りに関しては不明。
++++++++++++++++++++++++++++++++++++++++