Electric Stimulation: “Blood Pressure Adjustment Takes Time”
03/22/2013
Doctor Rolf Wachter; © private
Electric stimulation is the artificial activation of nerves through electric current. The most widely known example from medicine may be the cardiac pacemaker. But chronic high blood pressure can also be treated with an active implant: the baroreceptor stimulator triggers a stimulus in the nervous system that causes a drop of blood pressure.
MEDICA.de spoke with Doctor Rolf Wachter from the University Medical Center Göttingen. The hospital participates in a study to test the second generation of baroreceptor stimulators. A novelty here is the use of the device to treat chronic cardiac insuffiency.
MEDICA.de: Doctor Wachter, how does the baroreceptor stimulator work?
Rolf Wachter: The vascular surgeon attaches an electrode onto the carotid artery. The baroreceptor, a neural node that transmits stimuli to the brain to control the blood pressure is located there. The brain then causes a reaction in the autonomic nervous system, which regulates blood pressure. In our case, heart rate and blood pressure then decrease. The stimulator that is implanted under the collarbone amplifies the signal of the baroreceptor to the brain and the blood pressure drops more. This is the so-called baroreflex.
MEDICA.de: When do you use the stimulator?
Wachter: Technically, the treatment is permitted for patients with refractory hypertension. That is to say, the blood pressure is more than 140/90 mmHg, even though the patient is taking at least three drugs to combat it. We proceed more restrictively and take considerably more difficult cases, because this involves surgery: a patient does not take three, but usually five to six medications to lower blood pressure without adequate effect. Together with the nephrologists, which are in charge of our hypertension outpatient clinic, we interdisciplinary decide which patients are suited for the treatment.
MEDICA.de: The current study in Göttingen has been in progress since March 2011. In addition, the stimulators have also been available for some time now in the U.S.
Wachter: At this point, we are not just using the stimulators in the study, but to some extent already in regular patient care, and we also implant the device outside of scientific projects. The second, smaller generation of devices has been in use since 2011.
MEDICA.de: What results do you achieve in the long run after the implantation?
Wachter: After approximately six months, we achieve a blood pressure reduction of 25-30 mmHg. The effect seems to remain constant longer, but there are also indications that the effect is getting stronger. However, about 20 percent of patients also benefit little or not at all from this treatment. These patients leave the study, when they believe the device does not help. This is why after four to five years, we only see those patients again, who respond well to the treatment.
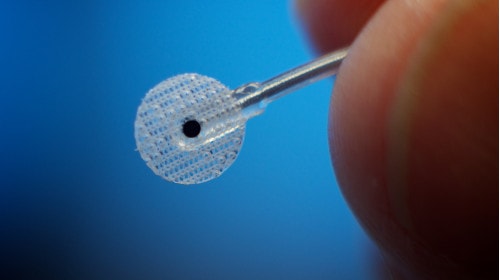
This tiny electrode is attached to the patient's carotid artery; © CVRxInc
MEDICA.de: Do you also notice side effects during operation?
Wachter: In individual cases, the baroreceptor stimulation is too strong and low blood pressure and heart rate cause problems. This can be resolved through reprogramming. In other cases, patients have become significantly calmer and more relaxed. We are currently trying to systematically analyze and understand such individual observations by extensively monitoring the patients. We pay attention to the heart, resilience, renal function and also to the psyche with the help of a psychosomatic specialist.
MEDICA.de: Why is patient monitoring so important?
Wachter: On the one hand, patients respond differently and on the other hand, the adjustment takes time. In one patient, the blood pressure could be lowered from 200 to 120 mmHg within minutes. If the body is no longer used to the low blood pressure, the sudden adjustment is problematic.
This is why patients in the beginning visit us monthly and we slowly increase the therapy. In addition, we check whether we are able to reduce drug use. For instance, what happens when we increase the stimulator output? Can we then reduce drug use? This takes time, which is why we monitor very intensely in the first six months. Afterwards, the intervals are getting longer, but patients still visit us several times per year.
MEDICA.de: Since the fall of 2011, you also treat patients with chronic cardiac insufficiency with the stimulator.
Wachter: This is still exclusively taking place as a study. So far, I am not able to say anything conclusive yet, but there appear to be similar effects than with high blood pressure. Definite results will be available in 2014 at the earliest.
MEDICA.de: How do you choose patients with cardiac insufficiency for the study?
Wachter: This is a clinical trial with strict criteria. We offer this therapy to relatively sick patients. These are patients undergoing standard therapy for systolic heart failure, who take ACE inhibitors, beta blockers as well as aldosterone antagonists, and who are still in class III of the NYHA classification and have already trouble breathing during light physical activity.