









私の外来には、胸壁の形に悩まれる患者さんが大勢、おいでになります。その中には他の病院で手術をお受けになった後に、「(初回の手術で入れた)バーを取り外してください」と言って手術をご希望になる方もおいでになります。
ご希望があれば手術は行っていますが、その際に、ちょっと気を付けなくてはいけない点があるのです。
多くの病院では「ナス法」という方法で手術を行いますが、ナス法で漏斗胸の手術を行う場合、術者はバーを胸郭に誘導しなくてはいけません。この時、バーは胸壁上のどこかのポイントで、胸壁を貫く必要があります。左右のそれぞれにこうしたポイントが存在します。この点は“ヒンジ・ポイント”と言われますが、バーはこの点で支えられています。
私はこの“ヒンジ・ポイント”が、なるべく内側の、乳頭のあたりに来るようにしています(図1)。力学的にバーを安定させるためには、そうすることが必要だからです(理由は別に書きます)。しかしこのようにバーをポジショニングさせるのは技術的にむつかしいので(これも理由は別に書きます)、“ヒンジ・ポイント”を胸壁の外側(脇の下くらいの位置)に設定する外科医が、実にたくさんいます(図2)。


図1:正しいバーの入れ方 図2:誤ったバーの入れ方
そうするとバーを抜去する際に、ちょっと気を付けなくてはいけないのです。バーはU字型をしていますが、これを抜く際には、まっすぐに曲げ直さなくてはいけません。ただ、外科医が直接、操作を行うことができるのは、“ヒンジ・ポイント”より外側の部分だけなのです。なぜなら、バーのうち、胸郭(「あばら」)に潜っている部分に対しては操作ができないからです。
“ヒンジ・ポイント”を内側に設定した場合には、U字型のバーを、ほぼまっすぐにすることができます。バーのかたちをまっすぐにしておけば、「スッ」とバーを抜くことができます。
しかし最初の手術で、バーを挿入した位置が外側すぎる場合には、バーを完全にまっすぐにすることはできません。外科医が曲げることができるのは、胸壁の外の部分だけです。ゆえに、なるべくまっすぐにしようと思っても、図に示したように“W”型にすることしかできません(図3)。
この状態でバーを引き抜くとき、“W”の角で心臓が押されます。バーのエッジはなめらかですから、仮にバーがそのように心臓を押したとしても、心臓が傷つくことはまずないでしょう。しかし一時的にせよ、心臓が圧迫されることは、やはりよくありません。私の患者さんの中には、他の病院で手術を受けられたあとに(その結果に満足せず)修正を求めてこられる方がたくさんおいでになります。正しい理論に沿って手術が行われていない患者さんに対してリカバリーをするのは多かれ少なかれ苦労するのですが、今日はその一つの理由をご紹介しました。
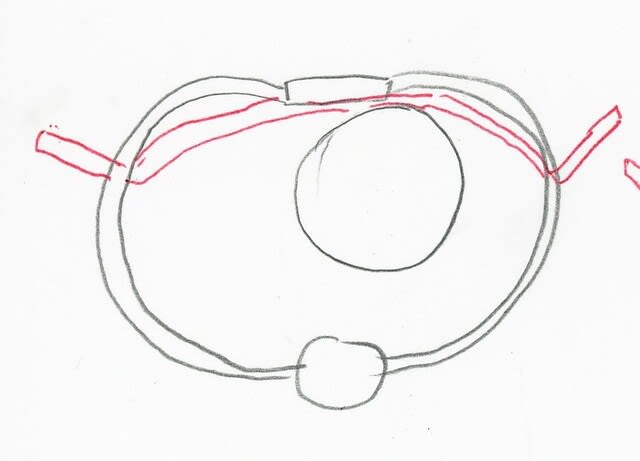
図3:”W”型に曲げざるを得ない 図4:抜去の際に、心臓を圧迫する
Many patients request that I correct their chest shapes after they receive surgery at other hospitals. These requests often annoy me, because re-correction of thorax shape is much more difficult than to achieve good results with the first operation. The readers might understand the difficulty, by assuming themselves as carpenters. A client comes to you and says, “I’ve had my house constructed, but I’m not satisfied with it. It’s neither as gorgeous nor as comfortable to live in as I had expected.” The person requests you rebuild the house. I believe you can easily imagine that such correction is much more challenging than building a house from scratch. To deepen your comprehension, I’ll provide more minute explanation by referring to actual problems I’ve encountered.
A 45-year-old male patient received surgery at a private hospital in Shikoku to correct his pectus excavatum. A correction bar was placed in his thorax in the primary surgery. He requested that I remove the bar. I asked why he didn’t ask the surgeon who had done the initial surgery to remove the bar. The patient said he was not satisfied with the hospital. “In particular”―he said―“The surgeon didn’t pay attention to pain control. I had terrible pain for several days and asked the surgeon to relieve it. However, he only prescribed suppositories. They didn’t work at all!”
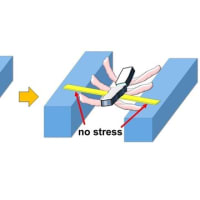
I explained to him, “Some of your ribs and cartilages were bent in the first operation. So, it is natural that you had pain in the previous operation. However, the secondary operation is another story. The shape of your chest wall has already stabilized. Simply removing the bar won’t cause stress on your bones and cartilages. Therefore, it is unlikely that you will have as intense pain as after the initial operation, even if the surgeon doesn’t take enough care. I recommend you ask the surgeon to remove his bars.”
Nevertheless, the patient insisted to receive operation at my hospital. So, I decided to work on him. I completed the second operation successfully, but I encountered a minor problem due to incorrect positioning of the bars in the first operation. In my method, I place bars so that the bars rest on ribs at their most anterior points (Figure 1).
However, the bar had been supported at points much lower and much more outside than I would place them (Figure 2). When placed this way, the bars aren’t dynamically stable (I’ll explain the reasons in another column). Besides the dynamic instability, placing the bars like in Figure 2 increases the risk in bar removal. In Figure 2, the bar penetrates the thorax at lateral points. The parts of the bar between its ends and these points exist outside of the thorax.
When surgeons remove correction bars, they first straighten the bar before removing it. The surgeon cannot work on the part of the bar inside of the thorax. It is only the part outside of the thorax that the surgeon can bend. So, the surgeon cannot make the bar completely straight. After being bent, the bar takes a shape similar to that of “W” (Figure 3). This shape is not ideal in removing the bar, because it presses on the heart in the process of the removal (Figure 4). The heart may very rarely be hurt. Nevertheless, I believe even such tiny risks should be avoided.









※コメント投稿者のブログIDはブログ作成者のみに通知されます