








Though many surgeons in Japan provide surgical treatment to patients with deformed chests, or pectus excavatum, they don’t necessarily do operations using current best practices. I often enlighten such surgeons with lectures at academic meetings, scientific papers, and articles at web sites like this.
In this article, I explain how we should work on the sternum. The sternum is the bone at the center of the chest. The sternum takes different shapes between adults and children.

These two images represent typical structures of the sternum in adults and children. The left image is that of an adult patient. Pay attention to the shape of the sternum. It is a single, unified plate. On the other hand, the sternum in the right image consists of four segments. This is a typical pattern for child patients. Let’s consider how this structural difference affects the operation.

This figure demonstrates the basic principle of the operation. First, the concave chest wall is elevated. Then metal plates are placed underneath the elevated chest wall to keep it at the corrected position. When operating on child patients, it is not so hard to elevate the chest wall, because the sternum is flexible.
The following images are the pre- and post- operative shapes of a child patient’s chest. Note the segmented sternum in the left image. The segments are connected with joints, and the sternum is flexible. So the chest wall can be elevated easily.

With child patients, thanks to the flexibility of the chest wall, we don’t need to cut any bones. We can correct the chest wall by simply placing one or two bars. The insertion can be done through short skin incisions.
In summary, the chest wall of a child patient is soft because of the flexibility of the sternum. Therefore, the chest wall can be elevated with little force. The only thing the surgeon should do is to place bars to keep the elevated chest wall at its correct position. So the operation is easy and can be done through short skin incisions.
However, adult patients are quite different stories. Although a considerable number of surgeons use the same technique for adult patients as that for child patients, this is problematic. Direct application of the technique for child patients to adult patients often causes trouble.
For instance, a patient recently requested I perform secondary treatment. She had received surgery at a university hospital in Tokyo. Although her chest shape improved to some extent with the first surgery, she was not happy, because she was annoyed by serious pain after the operation. I took computer tomography images of the patient including the one on the right side of the following figure. I wanted to know how the shape of the chest wall had been changed by the first operation. To evaluate the morphological change, I requested the surgeon who had done the previous operation to provide me preoperative images of the patient. He agreed and sent me preoperative images. The left side is one of those images. The right side is one of the postoperative images we had taken at our hospital. The shape of the chest wall appears to have improved.

However, the patient had been annoyed by serious pain. From immediately after the operation, the pain had persisted for more than 6 months, when she visited me seeking treatment.
Looking at the images, I found the surgeon who had done the operation had simply applied the method for children directly to this patient, though she was in her forties.
I explained why surgeons should not apply child-appropriate technique directly to adult patients, showing the picture given below: Adults’ sternums are hard and inflexible. Furthermore, the ribs attached to the sternum are much harder than those of children.
Therefore, when surgeons correct the shape of the adult chest wall, they have to pull it up forcibly. Accordingly, the elevated chest wall tends to go back to its original, concave position. The bar supporting the chest wall is strongly pushed downward, producing intense stress at the points where the bar and ribs intersect. This stress naturally causes pain. This is how postoperative pain develops in adult patients in cases where they are treated with techniques for CHILD PATIENTS.

The images of the above figure were those of another adult patient. Pay attention to the ribs supporting the bars. They had sagged toward the back. This finding supports the above-stated theory. 
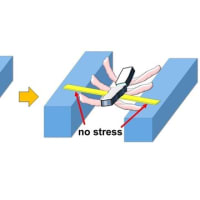
Then, what should surgeons do to avoid such problems? Several techniques are available. One such technique is to make the sternum flexible by dividing it. After the sternum is divided, the chest wall can be elevated with less force, producing less counter-stress on the bar. So, the patients are less likely to feel pain.

The following images are those of a patient in whom we divided the sternum to make it flexible. The divisions reduce the stress from the bars.









※コメント投稿者のブログIDはブログ作成者のみに通知されます